
MSK LAB 7A – Ungulate highlights of the Thoracic Limb
Learning Objectives
- Identify the anatomy of the carpal canal
- Identify the tendons and ligaments of the metacarpal region
- Identify the accessory ligaments of the digital flexors of the horse
- Identify bursae and tendon sheaths as noted
- Identify joint related anatomy of the carpus and fetlock
- Identify the ligaments of the digit as noted
Lab instructions:
Dissection teams are to dissect an equine thoracic limb, as provided on the day of the lab. Supplement dissection learning with liberal study and review of the limb models available in lab, wet and dry. Ruminant thoracic limb highlights should be studied on prosections and models.
Dissect: Firstly, review the cutaneous structures notable on the limb – chestnut and ergot for the horse. Take a moment to review the regions and joints of the limbs present.
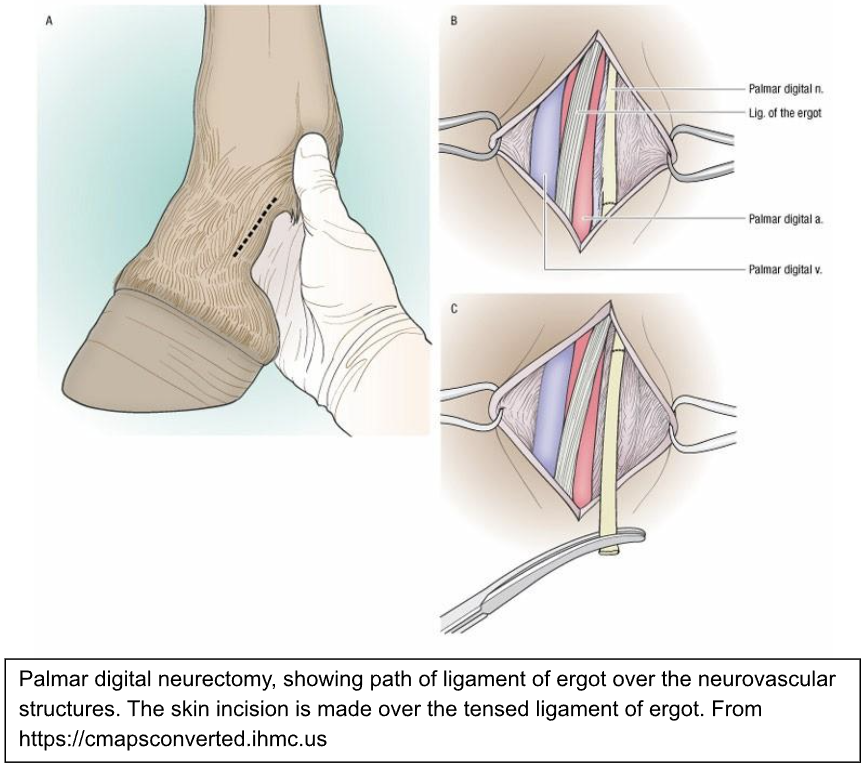
Horse note – a very thin, ligament of the ergot is present in the superficial fascia, passing from the ergot in a dorsal and distal (i.e. diagonal) direction over the palmar pastern. The left and right ligaments form an upside down ‘V’ configuration, with the V apex at the ergot. These thin bands can be highlighted by extending the foot and pushing the ergot proximally, to tense the palmar pastern soft tissues. See if you can appreciate them. Surgeons use this ligament as a landmark for a skin incision centered over the nerve, artery and vein (i.e. the neurovascular) bundle in the pastern, when performing a palmar digital neurectomy.
Moving on, make a skin incision on the medial aspect of the horse limb, extending to the hoof margin (the junction of skin with the epidermal hoof is called the coronet). Reflect the skin completely from the limb and discard it. Superficial vessels and nerves can be removed with the skin. Our focus is primarily on tendons, ligaments, bursa, and synovial structures.
Carpus: overview
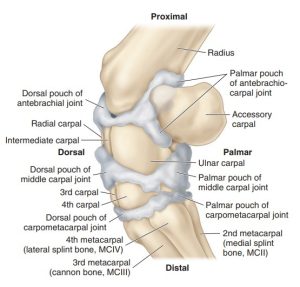
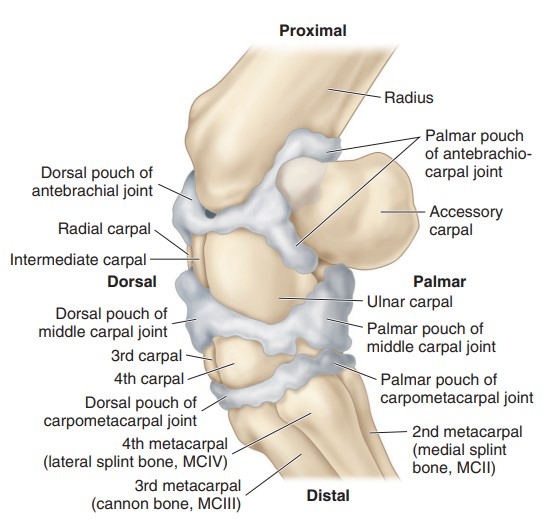
Recall from osteology and arthrology that the carpus is a construct of 3 major joints and numerous bones (dependent on species). The 3 joints are the antebrachiocarpal (often referred to as the ‘radiocarpal’ joint in equine), the middle carpal (often the ‘intercarpal’ in equine), and the carpometacarpal joint. The comparative bones of the carpus for our domestic species can be reviewed here.
Flexion of the carpus occurs at the antebrachiocarpal joint and the middle carpal joint. The synovial cavity of the antebrachiocarpal joint does not communicate with other joints, whereas the middle and carpometacarpal joints always communicate.
Powerful lateral and medial collateral ligaments of the carpus attach on each side to stabilize this complex joint that acts mostly in a dorsopalmar (axial) plane.
Dissect: Identify the location of the antebrachiocarpal joint, middle carpal joint, carpometacarpal joint, and the lateral and medial collateral ligaments of the carpus. If practical, firmly flex the carpus and palpate the dorsal spaces of the antebrachiocarpal and middle carpal joints, between the extensor tendons passing over the dorsal carpus. These spaces are sites of arthrocentesis.
-
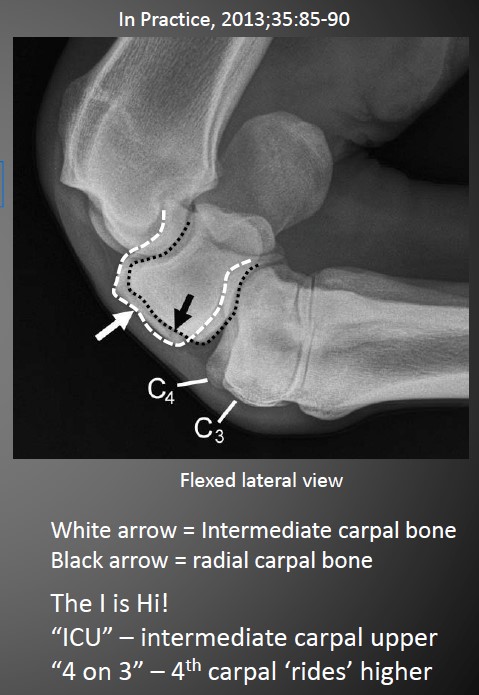
- Horse flexed carpus 9
-
-
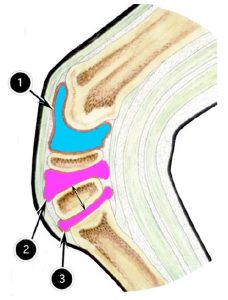
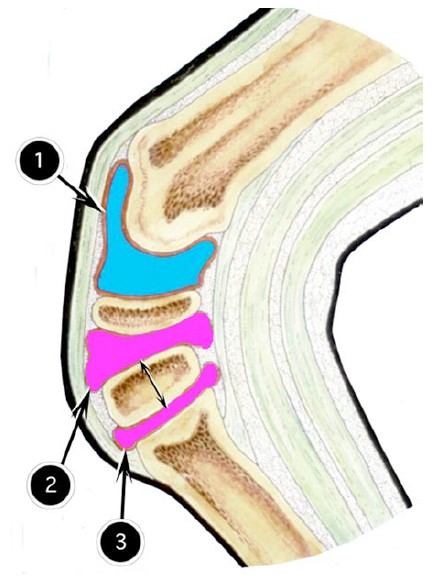
Schematic representation of equine carpal
complex, sagittal section: (1)
antebrachiocarpal joint cavity; (2) middle carpal joint
cavity; (3) carpometacarpal joint cavity. Doubleheaded
arrow indicates communication between 2 &
3.
-
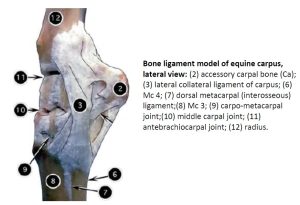
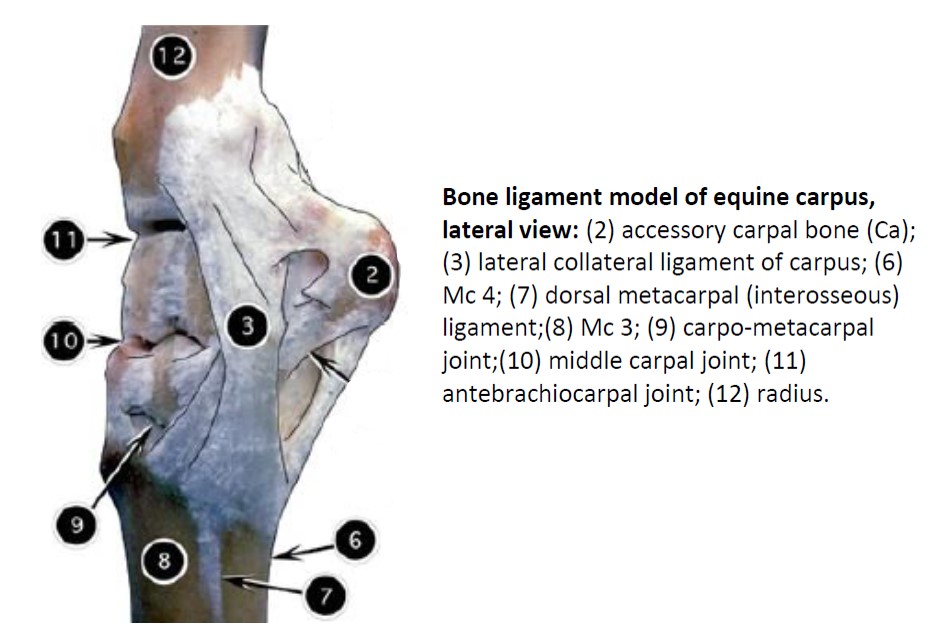
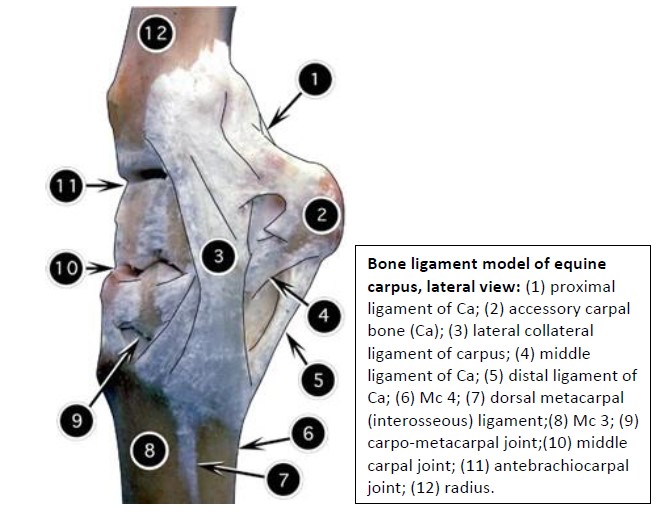
- Bone ligament model of equine carpus, lateral view. 2
-
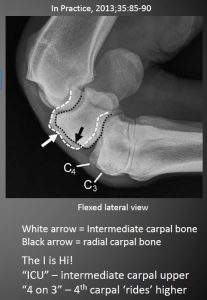
- Flexed horse carpus radiograph Dr. Nick Petrovitch
Clinical relevance: Arthrocentesis
Arthrocentesis (= inserting a needle into a joint) of the antebrachiocarpal and middle carpal joints is performed dorsally with the carpus held in flexion.
“Carpal hygroma” (aka Capped Knee) is an acquired subcutaneous fluid accumulation over the dorsal carpus that does not typically communicate with the joint spaces (but can!). The term carpal hygroma is loosely used to describe carpal swelling of many causes. The clinical work up must distinguish subcutaneous bursa, from tendon sheath, from joint sac. |
 |
Carpal canal
The carpal canal is the tunnel that accommodates the digital flexor tendons and certain vascular and nervous structures (species specific) as they traverse the carpal complex and continue on their way to the metacarpus. The canal is bound dorsally by the relatively thick palmar carpal ligament, which converts the irregular palmar surface of the carpal joint complex into a smooth track for the digital flexor tendons. The canal is bound laterally by the accessory carpal bone and palmaromedially by the flexor retinaculum of the carpus. A carpal sheath envelops the flexor tendons.
Dissect: Reflect and discard superficial and deep fascia (as was done on the carnivore limbs in Lab 5A) to help isolate and identify structures. Sharply transect the flexor retinaculum and retract its margins to open the carpal canal. Identify the flexor tendons present. Elevate the tendons and neurovascular tissues to visualize the palmar carpal ligament, dorsally. The carpal sheath was likely incised when the flexor retinaculum was cut. If not, open the carpal sheath now to appreciate its layer enveloping the tendons.
-

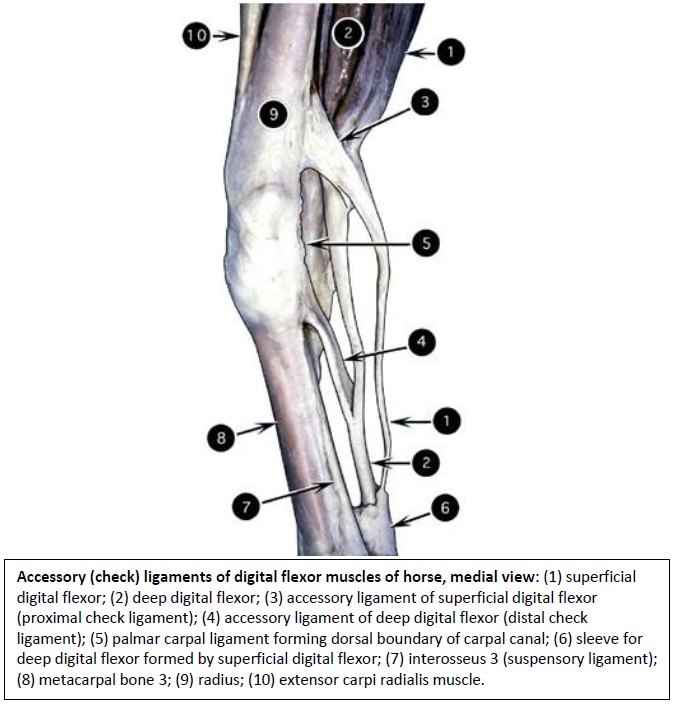
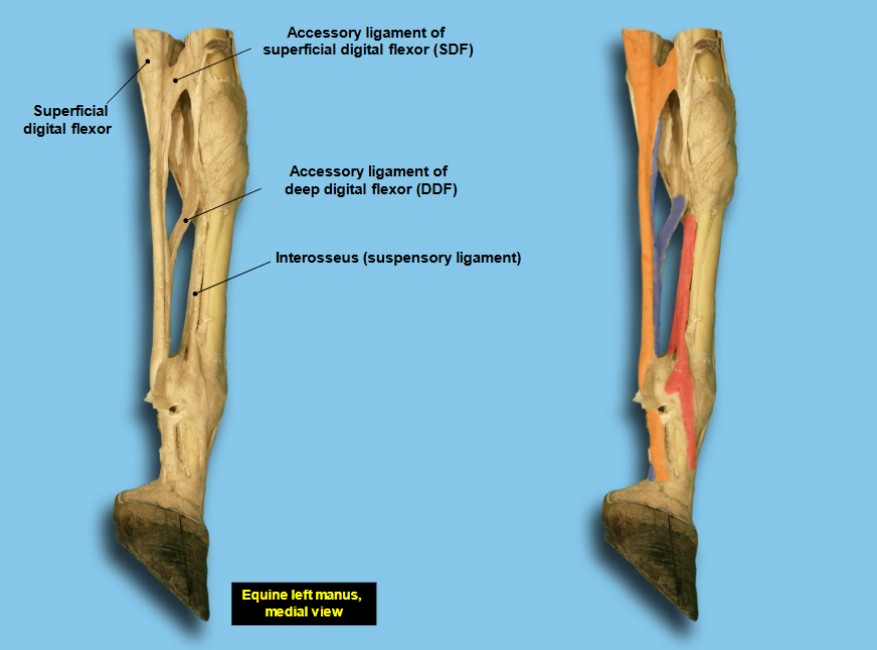
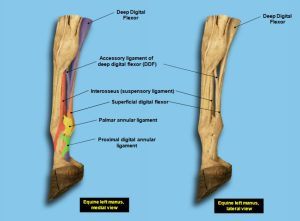
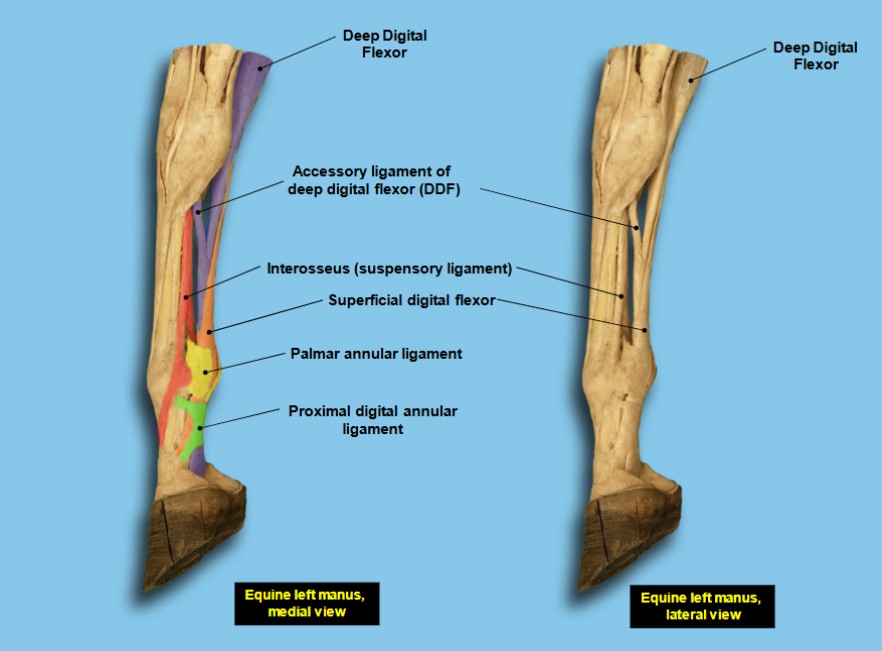
- Accessory (check) ligaments of digital flexor muscles of horse, medial view 2
-
-
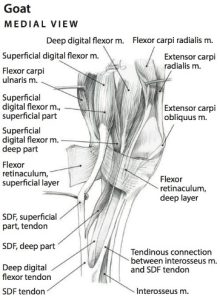
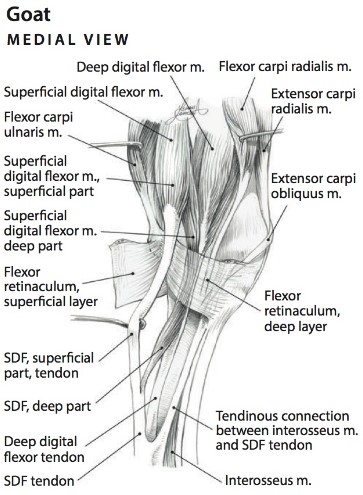
Muscles of the left carpal region of the goat, medial view (SDF—superficial digital flexor m.)
6
-
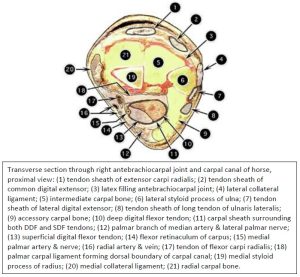
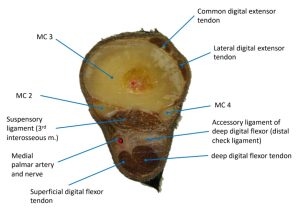
- Transverse section through right antebrachiocarpal joint and carpal canal of horse, proximal view 2
Clinical Relevance: carpal canal and carpal sheath
Teno/tendosynovitis of the carpal sheath; tenoscopy of the carpal sheath to diagnose and treat injury to the flexor tendons, to perform a proximal check desmotomy, to treat osteochrondroma of the distal radial physis.
FYI – Video of a check ligament desmotomy surgery – 6 min
-

- Before check ligament surgery

-

- 3.5 months after check ligament surgery

Metacarpus
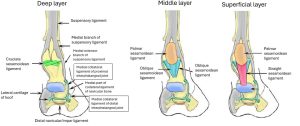
Before we dissect the limb further, let’s consider metacarpal bone ligaments in the horse.
Metacarpal bone ligaments – horse
Metacarpals 2 and 4 (medial and lateral splint bones) are attached proximally (i.e. at their base) by a set of interosseous ligaments to metacarpal 3 (cannon bone). Sometimes these ligaments, particularly the dorsal metacarpal ligament, are over-strained and torn, resulting in swelling and pain. Periosteal reaction to the trauma results in a bony ‘spot weld’ between the two metacarpal bones connected by the ligament. This bony callus is often visible. The injury and visible swelling (acute or chronic) is referred to as a “splint”.
Observe: Identify on prosections the dorsal metacarpal ligament (labeled 7 in image below).
Clinical Relevance: “splints”
“Splints”, the disease (not to be confused with the normal ‘splint bones’ i.e. MC2 and MC4).
-
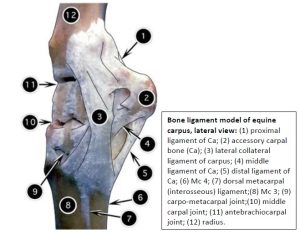
- Bone ligament model of equine carpus, lateral view
Dorsal metacarpal region
From the carpus, moving distally, on the dorsal surface, the tendons of the digital extensors track into the digits. Over the carpus these tendons, along with others, are wrapped in lubricating synovial tendon sheaths.
Dissect: Reflect and discard fascia, and then clean, isolate and identify the tendons of the common digital extensor and lateral digital extensor mm., following them into the digit(s). Incise their individual tendon sheath at the carpus to appreciate this structure.
Palmar metacarpal region
From the carpus, moving distally, on the palmar surface, the tendons of the digital flexors track into the digits. In addition, the accessory ligament of the DDF and the suspensory ligament are important features of this region, with species variation. We will consider these structures next.
3rd Interosseus m. aka Suspensory Ligament
Horse:
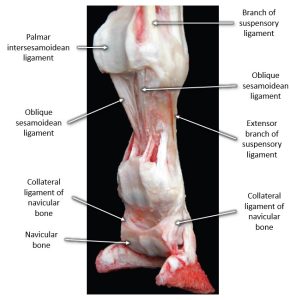
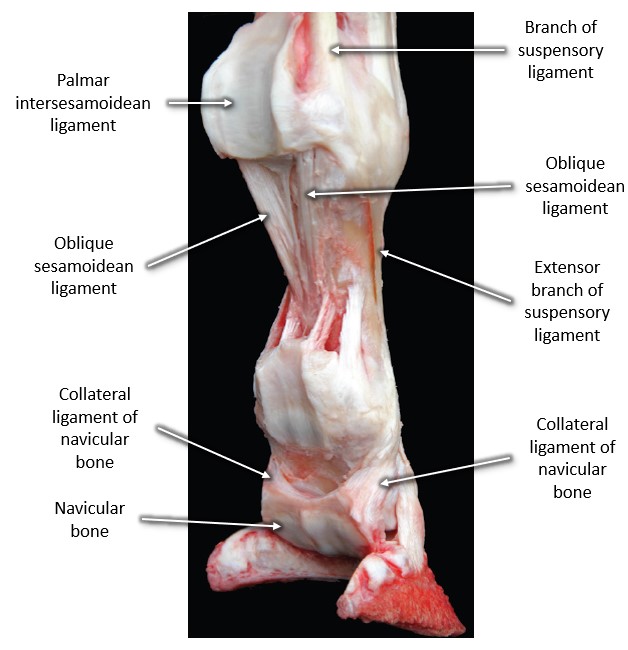
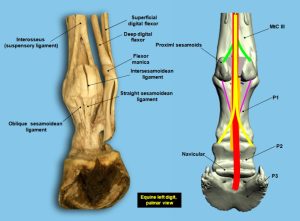
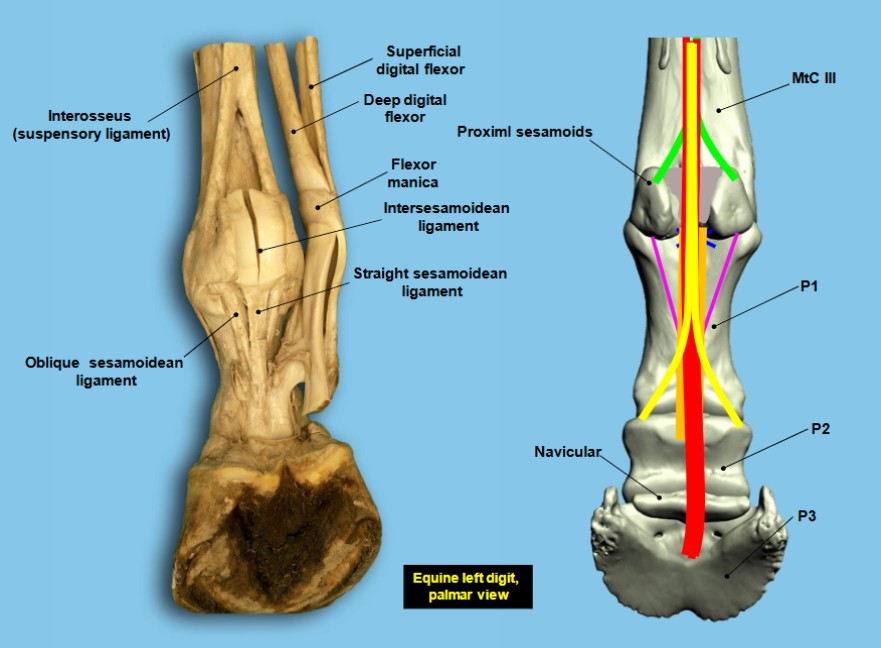
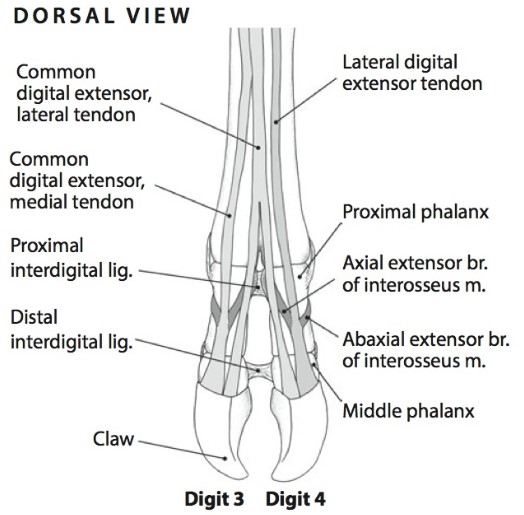
The 3rd interosseus m., more frequently referred to as the suspensory ligament, is primarily fibrous in the horse and arises from the palmar distal carpus and proximal metacarpus. In the distal third of the metacarpus the ligament divides into a strong lateral and medial branch. The branches attach to the abaxial surface of the respective proximal sesamoid bone. Lateral and medial extensor branches then continue the suspensory ligament from the sesamoids, passing obliquely to the dorsal pastern to join the common digital extensor tendon. These extensor branches are easily palpable in the live horse, along with the rest of the suspensory ligament.
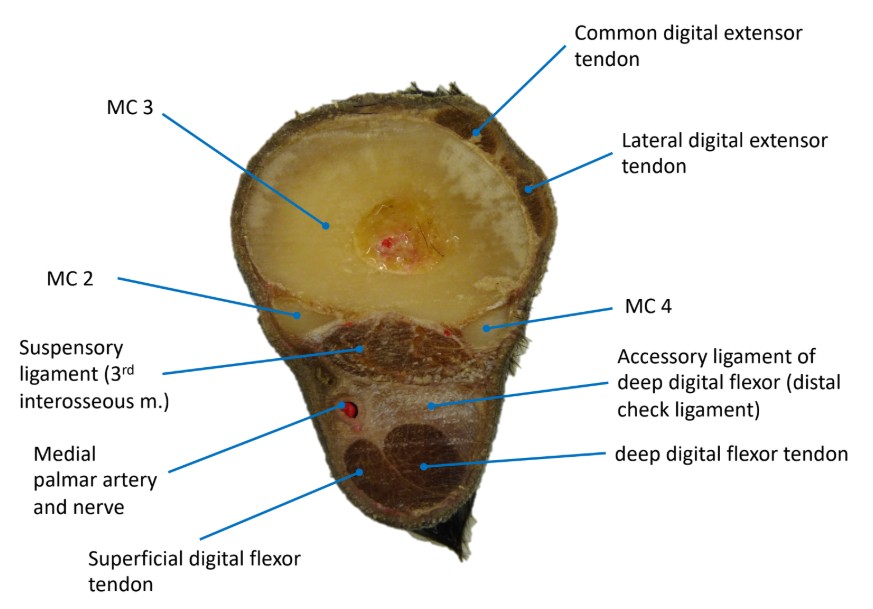
Dissect: Horse limb – remove fascia as necessary to clean, isolate, and identify the flexor tendons, the accessory ligament of the DDF (distal check ligament), and the more deeply located suspensory ligament in the palmar metacarpal region, to the level of the mid to distal metacarpus. View these structures on prosections too. When all is identified, name the 4 structures visible in the proximal half of the palmar metacarpus, in order, from superficial to deep (i.e. palmar to dorsal direction), as would be seen on an ultrasound of the region.
-

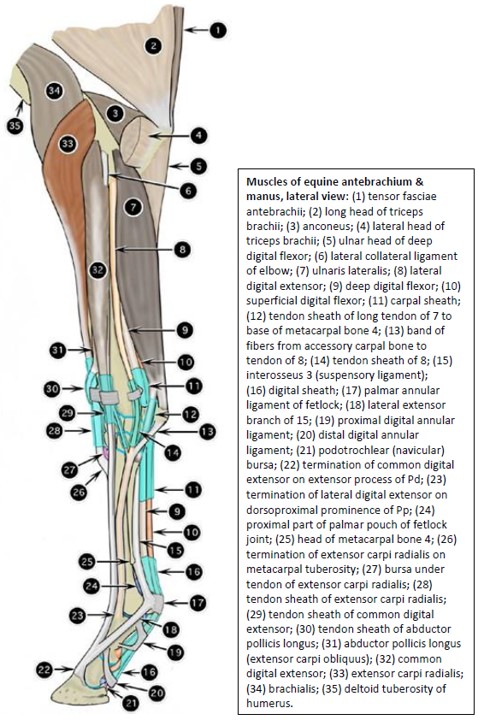
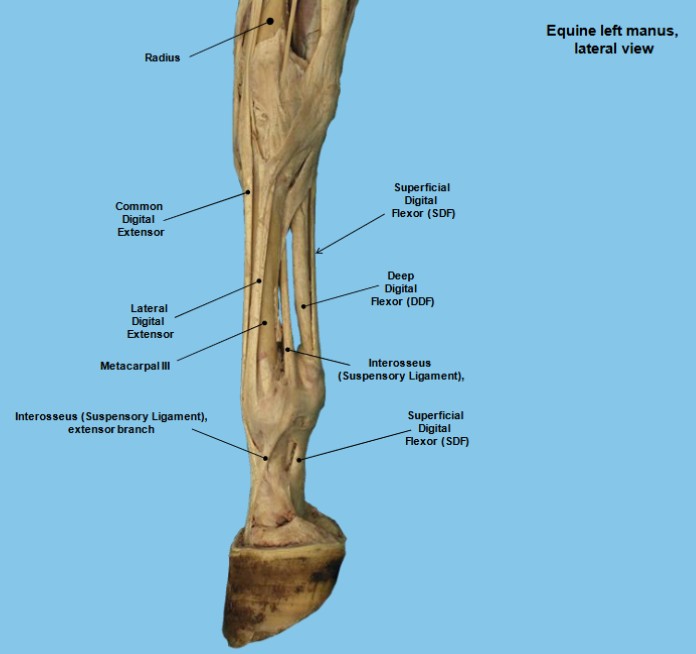
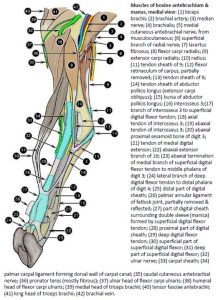
- Muscles of equine antebrachium & manus, lateral view 2
-
- Accessory (check) ligaments of digital flexor muscles of horse, medial view 2
-
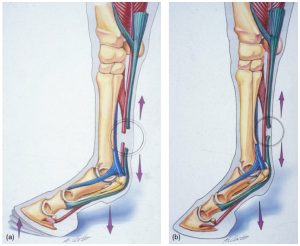
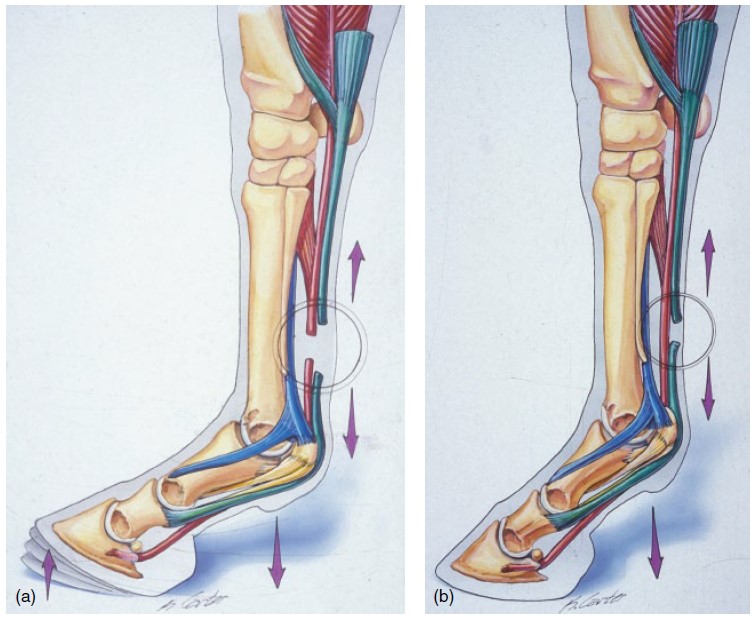
- Illustration of the biomechanical effects of lacerations of both the SDFT and DDFT (a) and just the SDFT (b) in horses with flexor tendon lacerations. 19
-
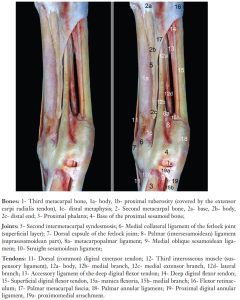
- Medial aspect of the horse metacarpus: right forelimb. 17
-

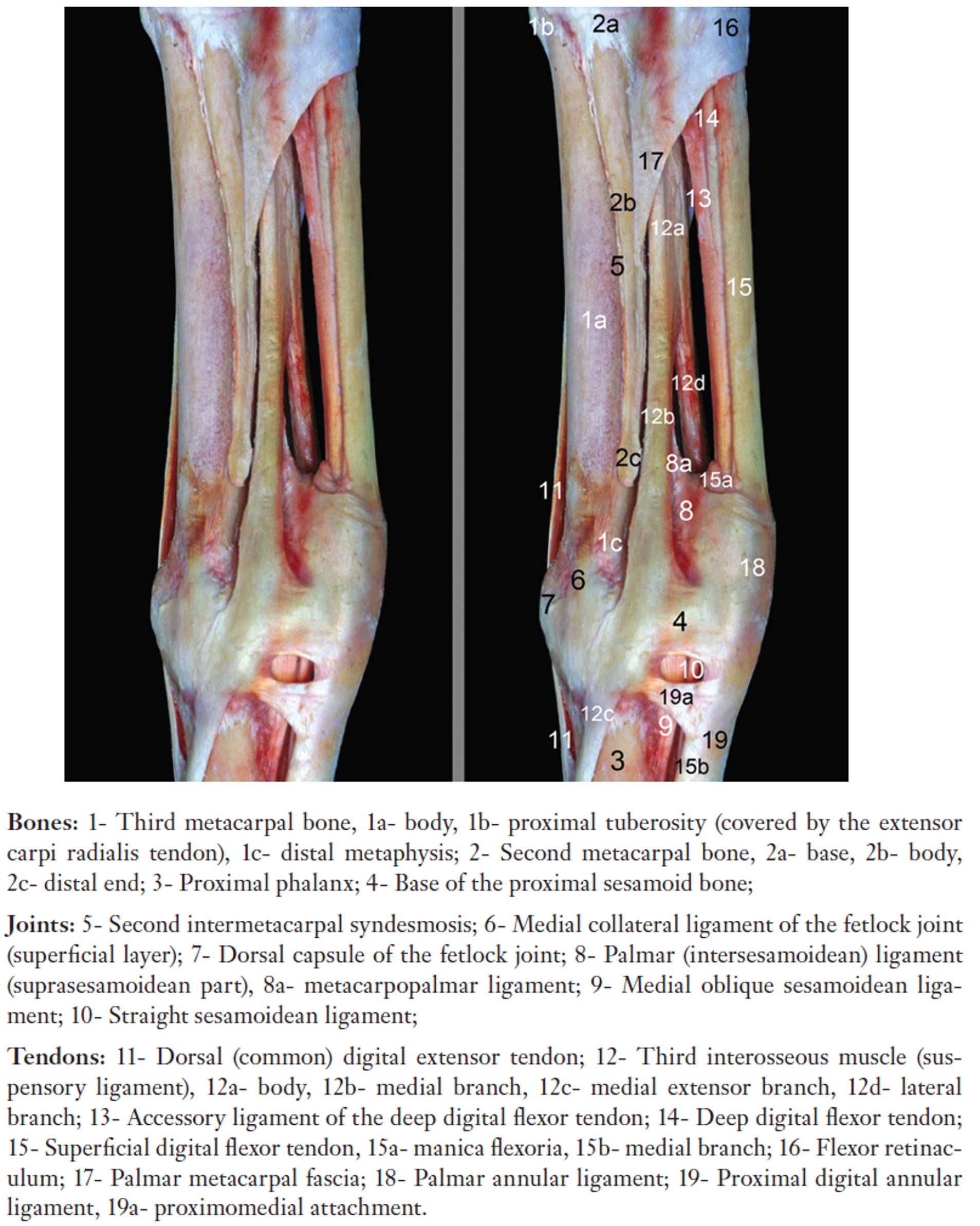
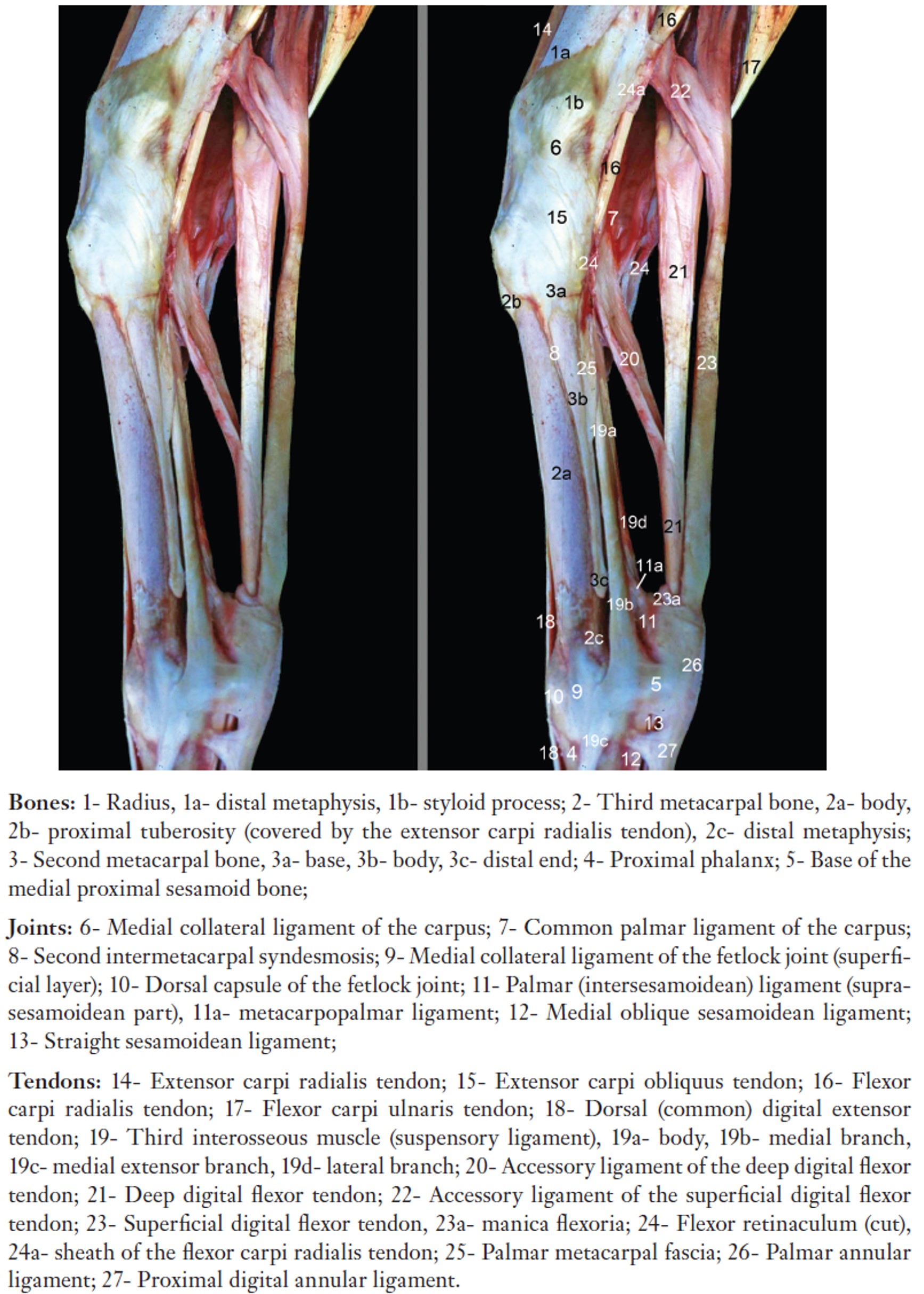
- Medial aspect of the horse metacarpus and adjacent areas, right forelimb. 17
-

- Horse suspensory ligament. 40
-
- Horse metacarpus. 40
-
- Horse metacarpus showing check ligament.
Clinical Relevance: Suspensory ligament
The suspensory ligament is an important component of the suspensory apparatus (see later) providing support to the palmar fetlock and digit; suspensory desmitis (in the body or branches) is a common cause of lameness.
Fetlock and digit – horse
Observe: Beyond your dissection specimen, many of the ligaments and tendons we want to identify in this next section can and should also be studied on prosected models.
Ligaments of ergot
We attempted to palpate these structures while the skin was still intact at the start of the dissection. Shiny, white, fine ligaments, subcutaneous in location, pass obliquely from the fibrous tissue deep to the ergot across to their distal attachments. They pass diagonally across the palmar digital nerves and vessels. The ligaments are about the same size as the nerves, and can be confused with them. The ligaments are a good surgical landmark for making the skin incision to perform a palmar digital neurectomy.
Observe: If still present after the skin removal, observe these minimally functional ligaments. Their primary relevance is for surgical landmark use, as already stated.
Clinical Relevance: ligaments of the ergot and palmar digital neurectomy
Surgical landmark for PD neurectomy surgery and not to be confused with the palmar digital n.
Fetlock joint
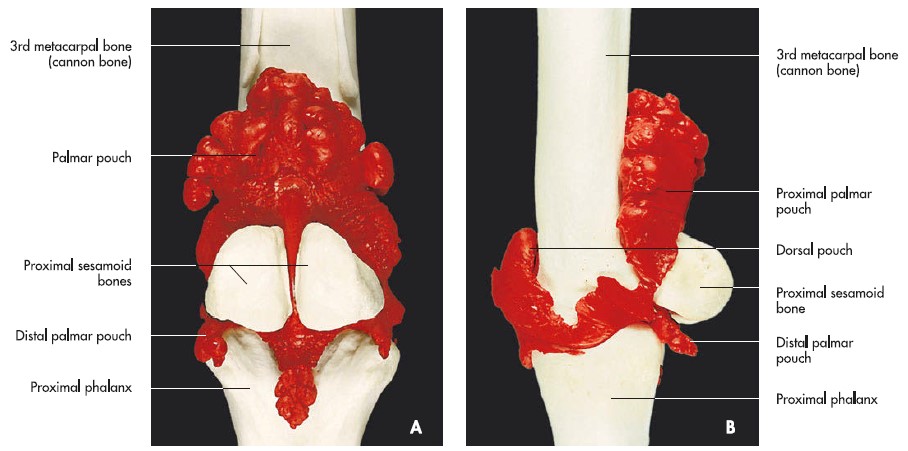
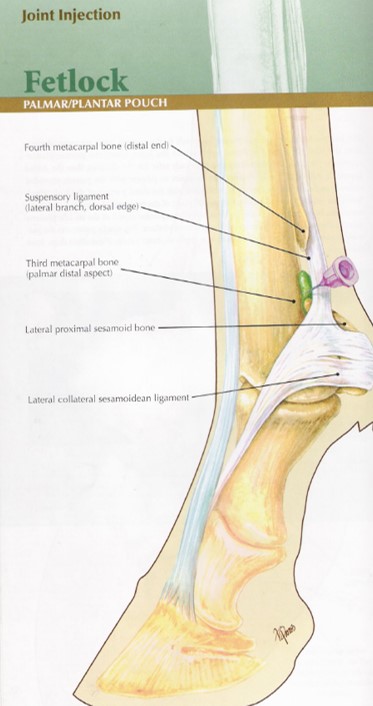
Observe: Laterally or medially, palpate the groove between the palmar surface of the cannon bone, the dorsal surface of the suspensory branch and just distal to the palpable button of the splint bone. This groove is the location of the palmar pouch of the fetlock joint. Be aware of this large pouch and that it lies dorsal to the palpable medial and lateral branches of the suspensory ligament.
Based on the location of the palmar pouch of the fetlock it follows that swelling of the fetlock joint is dorsal in location relatively to the suspensory ligament. The digital flexor tendon sheath (see later) and any swelling related to it lies palmar to the suspensory ligament.
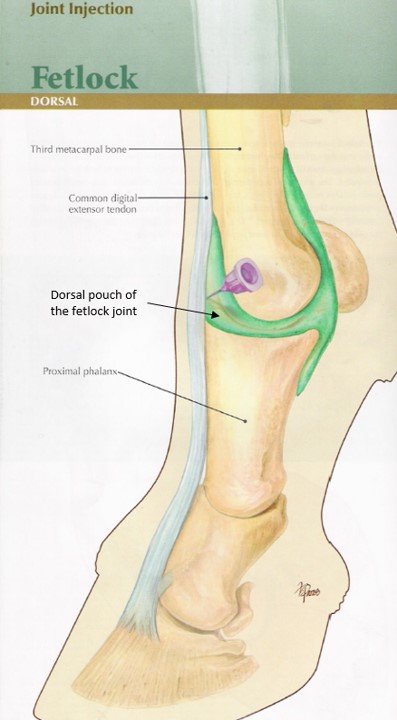
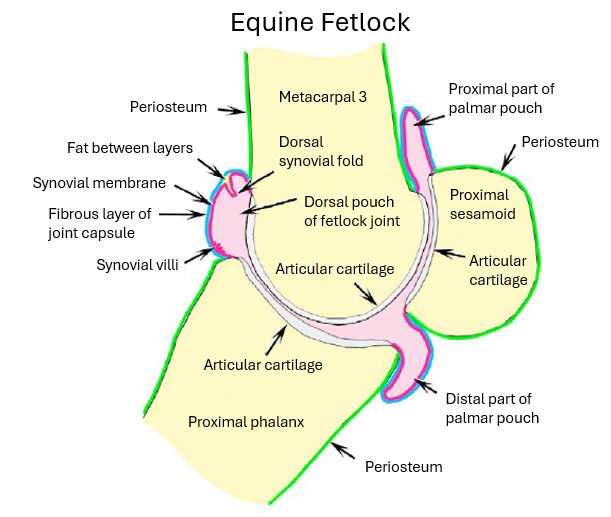
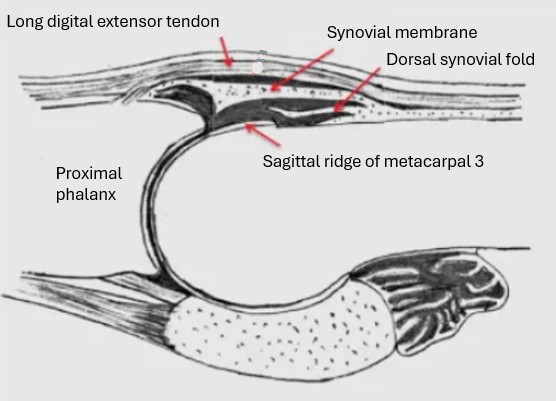
Dissect: Reflect the digital extensor tendons off the surface of the dorsal fetlock joint, transecting the tendons at the distal metacarpus if necessary. Open the dorsal pouch of the fetlock joint capsule by making a transverse incision. Examine the opened dorsal pouch of the fetlock joint. It may be possible to identify a normal synovial fold projecting from the proximal attachment of the joint capsule to the dorsal surface of MC3.
Clinical Relevance: synovial fold in dorsal fetlock joint pouch.
Villonodular synovitis (swelling of the dorsal synovial fold, causing lameness); arthrocentesis and arthroscopy of the fetlock is performed dorsally and palmarly.
-
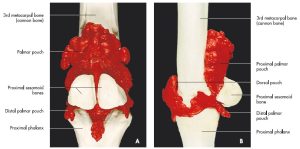
- Dorsal and palmar pouches of fetlock joint 7
-
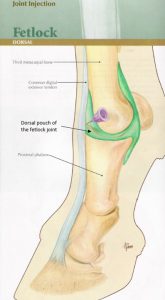
- Fetlock joint injection – dorsal 21
-

- Fetlock joint injection – palmar/plantar 21
-
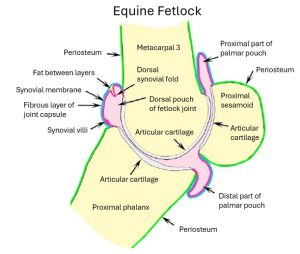
- Equine fetlock joint. 2
-
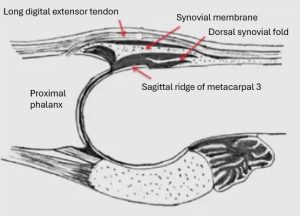
- Synovial fold of fetlock joint.
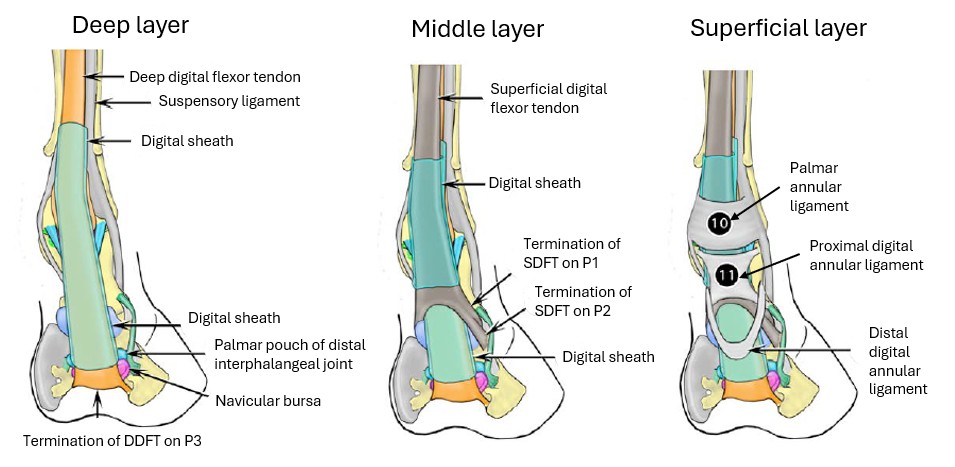
Digital flexor tendon sheath and digital ligaments
Remember, study prosections too, after completing the dissection. An important tendon sheath and a series of ligaments are to be identified in this section.
A synovial sheath, the digital flexor tendon sheath, envelops the DDF and SDF tendons in the distal fourth of the metacarpus and extends distally to the distal pastern region. Synovial effusion of the digital flexor tendon sheath may be referred to as ‘wind puffs’ and this can be observed after a horse has vigorously exercised, secondary to a mild digital tenosynovitis, or effusion may be present on a more chronic basis, once it develops.
Dissect/observe: Picking up from where left off, continue separating the SDFT from the DDFT in the distal metacarpus. As the tendons are retracted apart the digital flexor tendon sheath will be opened, if it is not already from previous dissection.
Grasp the flexor tendons and retract caudally and note they are ‘strapped down’ to the palmar aspect of the fetlock joint.
The tendons are held in position on the palmar fetlock by the palmar annular ligament of the fetlock. Much like a retinaculum, the palmar annular ligament retains the tendons in the channel created by the proximal sesamoid bones.
-
- Equine digital region, caudomedial view. 2
-
- palmar annular ligament. 40
Clinical Relevance: digital flexor tendon sheath
Digital sheath tenosynovitis; avoidance of sheath when doing perineural blocks; tenoscopy of sheath to do a palmar annular desmotomy.
Clinical Application: Q4
Review the image. Where is the swelling focused? What is a common term for this swelling?
What structure is swollen? (Photo credit: Gary Baxter).

(Answer)
Distal to the palmar annular ligament of the fetlock, the flexor tendons are retained by the proximal and distal digital annular ligaments against the palmar pastern. The gap between the proximal and distal digital annular ligaments is the lowest available access site to the digital flexor tendon sheath of the horse on the palmar/plantar distal pastern [palpation of this area is routine and if detect a sponginess it may mean increased synovial fluid is present in the digital sheath].
Dissect: Carefully, vertically transect the palmar annular ligament on its lateral margin, being sure to be palmar to the neurovascular bundle passing over the medial and lateral fetlock. With the ligament transected the exposed flexor tendons traveling across the fetlock within their synovial sheath are identifiable. Moving distally into the pastern, identify and transect the digital annular ligaments (may be hard to appreciate, they are no more than fascial thickenings) along their lateral margin to further open the digital flexor tendon sheath and to follow the flexor tendons.
Back at the fetlock, the SDFT forms a complete sleeve around the DDFT. This is called the proximal manica flexoria. This structure can tear and be a cause of lameness in horses.
-
- Equine digital region, caudomedial view. 2
-
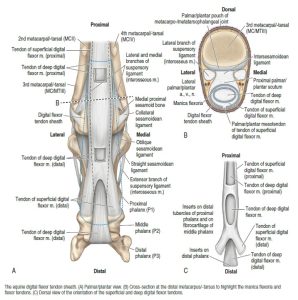
- Equine Digital Flexor Tendon Sheath 9
-
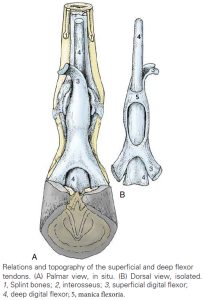
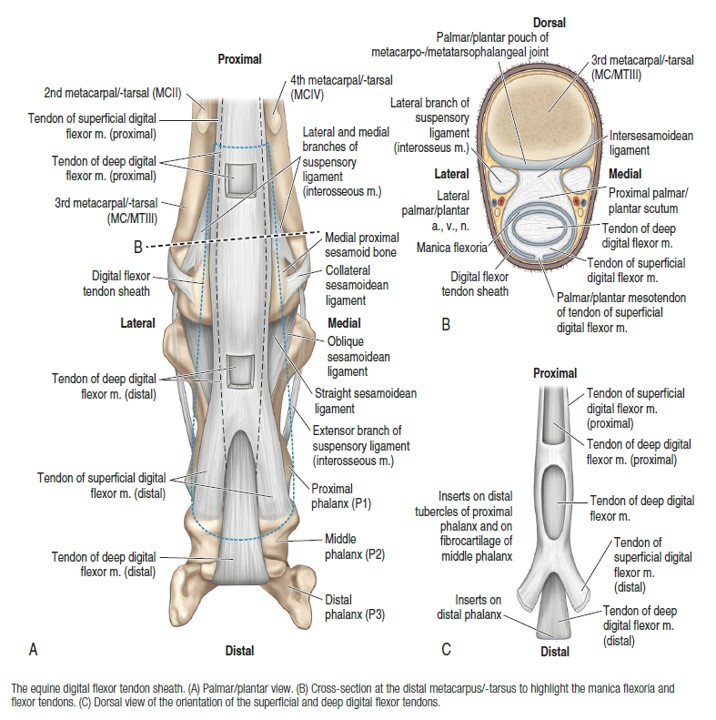
- Relations and topography of the superficial and deep flexor tendons. 8
Observe: Examine the flexor tendons and identify this sleeve. FYI – there is also a clinically described smaller, distal or digital manica flexoria in the mid pastern.
In the proximal pastern the SDFT must assume an abaxial position to the DDFT so it can insert on the proximal (Pp) and middle (Pm) phalanges (in the horse, and only the middle phalanx in the ox) while the DDFT continues on its axial path to the distal phalanx (Pd).
Observe: Separate the SDFT and DDFT in the proximal pastern. Note how the SDFT divides and passes to the sides of the DDFT (contributing to the smaller sleeve around the DDFT at this level i.e. the distal manica flexoria). (FYI – formation of the manica flexoria in the ruminant is supplemented by contributing branches from the interossei mm.)
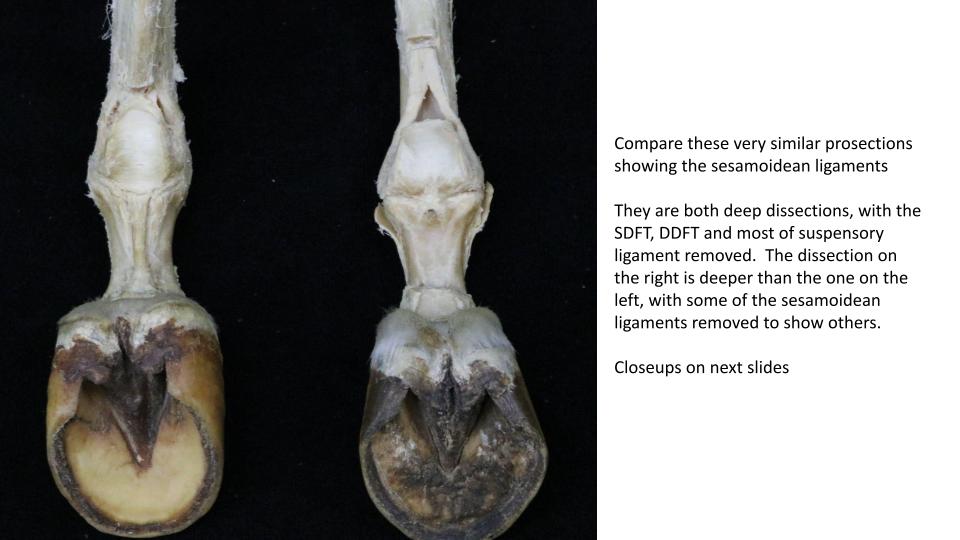
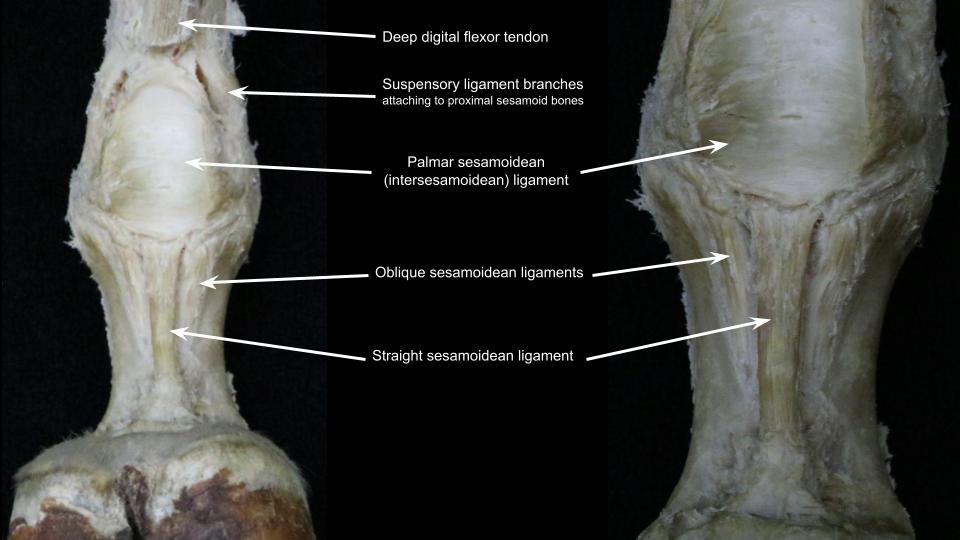
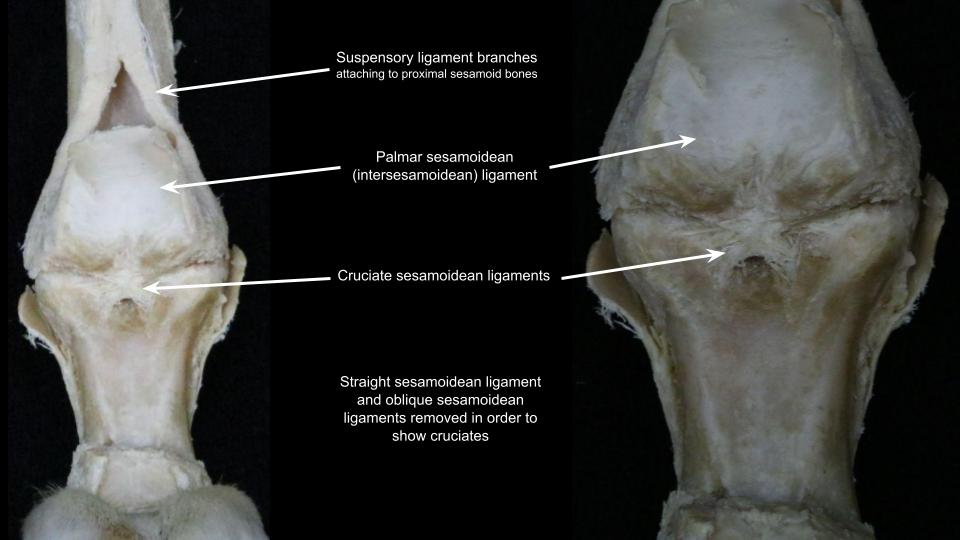
Dissect: Retract the flexor tendons from their pathway across the palmar fetlock and examine the palmar sesamoidean (aka intersesamoidean) ligament, which is connecting between the proximal sesamoid bones and extending proximally as a fibrocartilaginous gliding and bearing surface for the flexor tendons (this extension is called the proximal scutum). Review this ligament on prosections too.
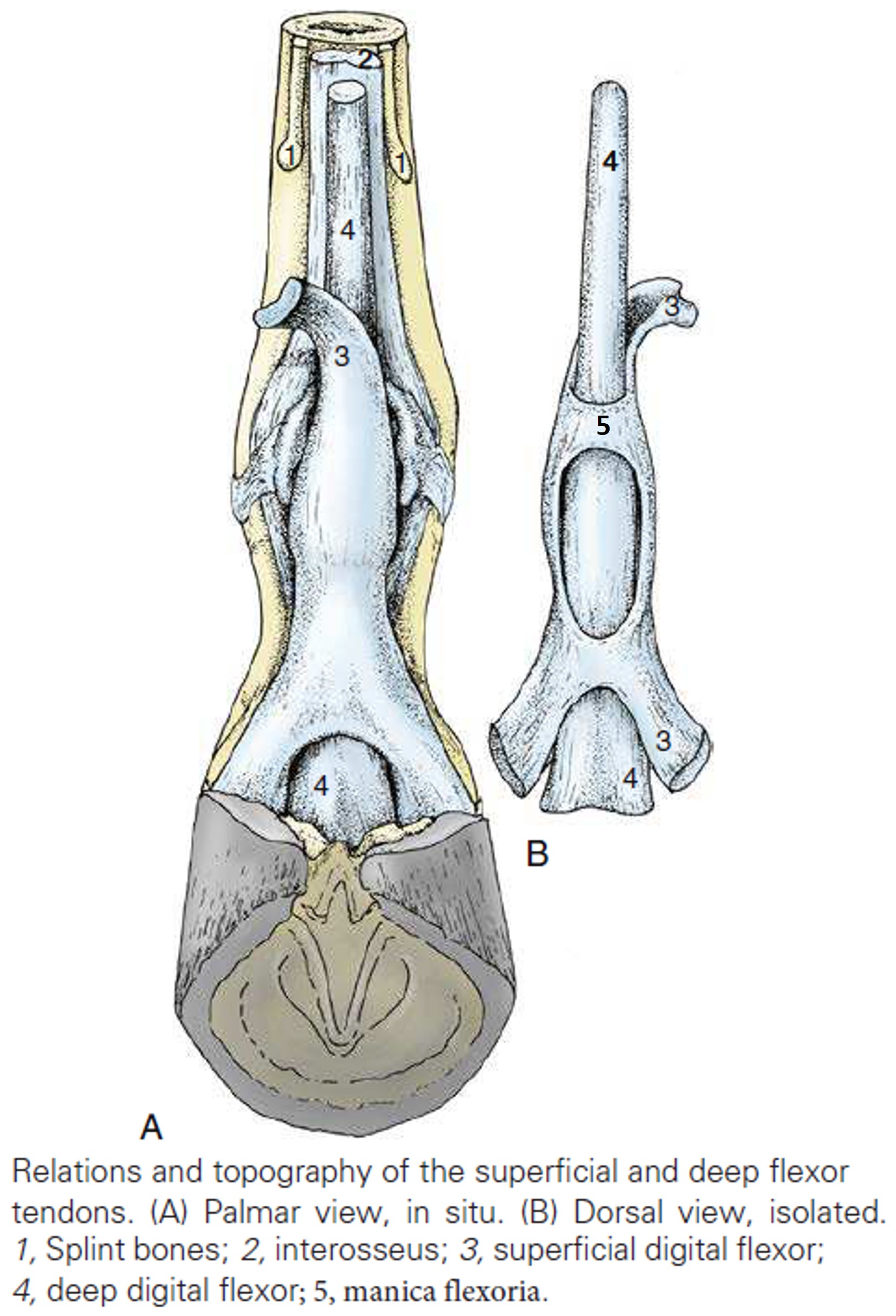
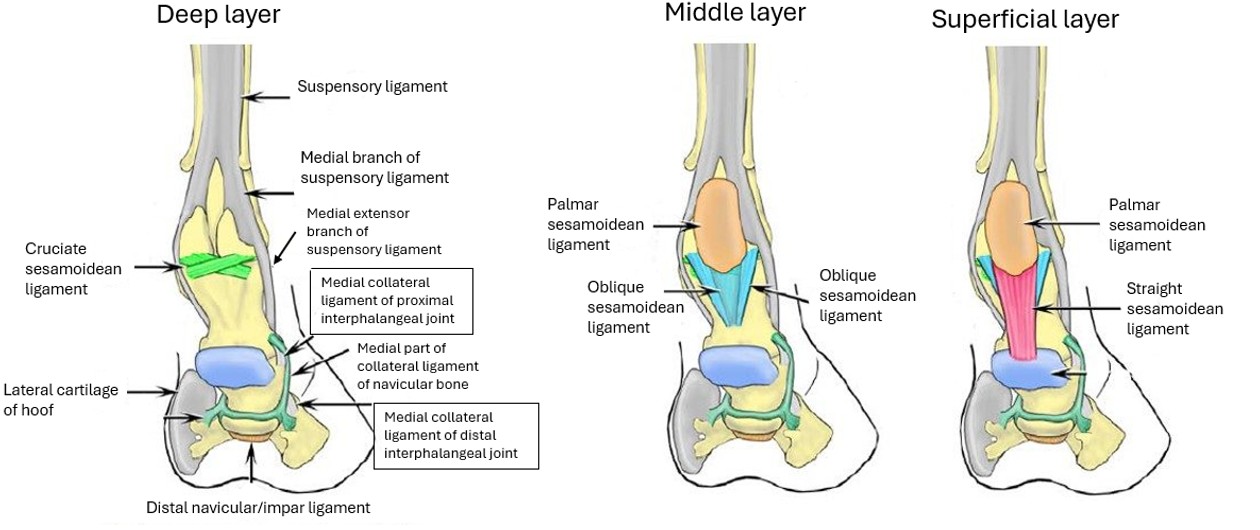
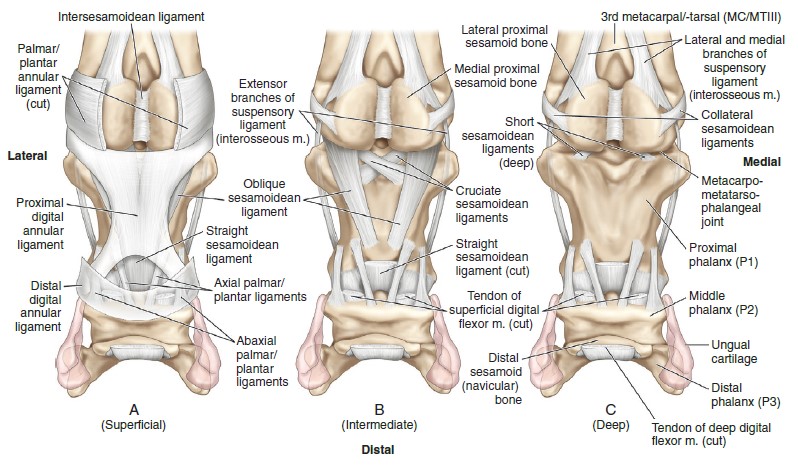
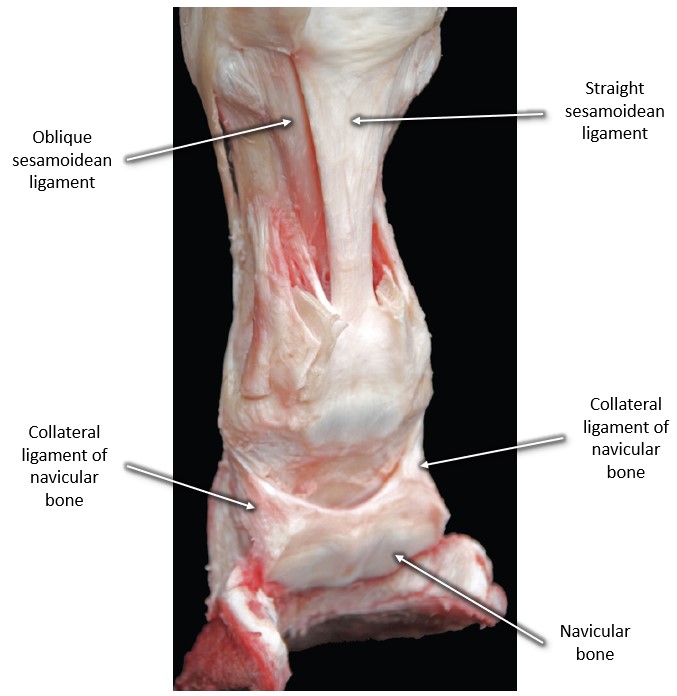
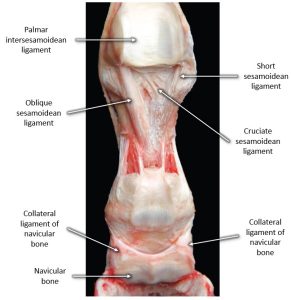
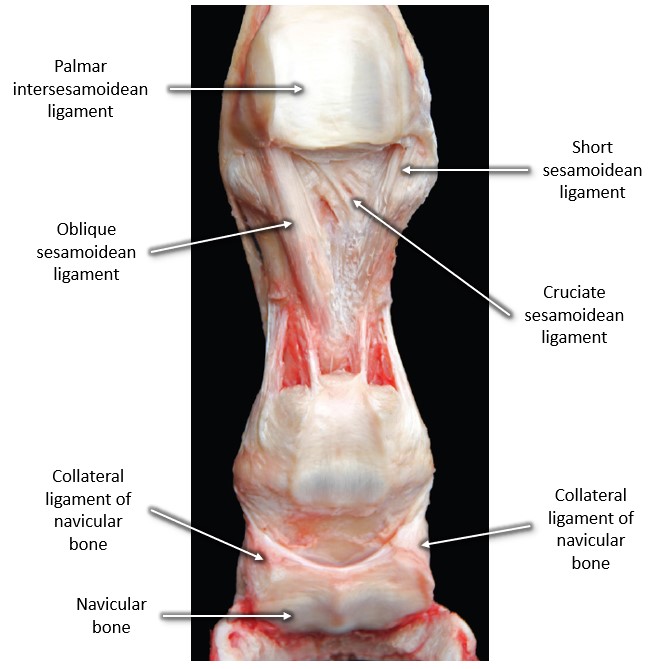
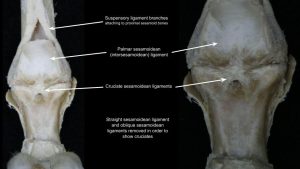
Recall the suspensory ligament branches attach to the abaxial surface of the proximal sesamoid bones, and then extensor branches pass dorsally to insert into the common digital extensor tendon. Distally the proximal sesamoid bones are anchored to Pp and Pm by a quartet of (distal) sesamoidean ligaments (straight/superficial, oblique/middle, cruciate/deep, and short sesamoidean ligaments).
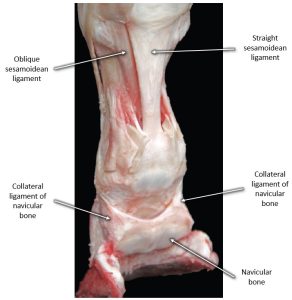
Dissect: Transect the digital flexor tendons at the mid to distal metacarpus level and retract the tendon stumps distally. Identify the straight sesamoidean ligament, then, if necessary, transect this ligament close to the proximal sesamoid bones and elevate it to get a better view of the oblique sesamoidean ligaments lying a little more deeply on each side. For all these ligaments (including cruciates and shorts), examine prosections.
-
- Equine Suspensory Apparatus and Other Ligaments; Caudomedial View. 2
-
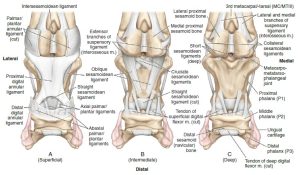
- Palmar plantar View of the Distal Sesamoidean Ligaments of the Equine Limb. A. Superficial. B. Intermediate. C. Deep. 9
-
- Palmaromedial aspect of the right digital area of the horse after removal of the flexor tendons. 17
-
- Palmarolateral aspect of the right digital area of the horse after removal of the flexor tendons and straight sesamoidean ligament. 17
-
- Palmar aspect of the right digital area of the horse after removal of the flexor tendons as well as straight and lateral oblique sesamoidean ligaments. 17
-
- Horse sesamoidean ligaments40
-
- Horse sesamoidean ligaments
-
- Horse sesamoidean ligaments
-
- Horse sesamoidean ligaments
Clinical Relevance: sesamoidean ligaments
At this point there is no more dissection to be done and content is learned on prosections.
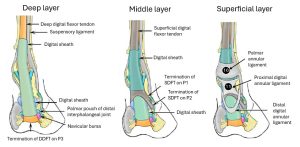
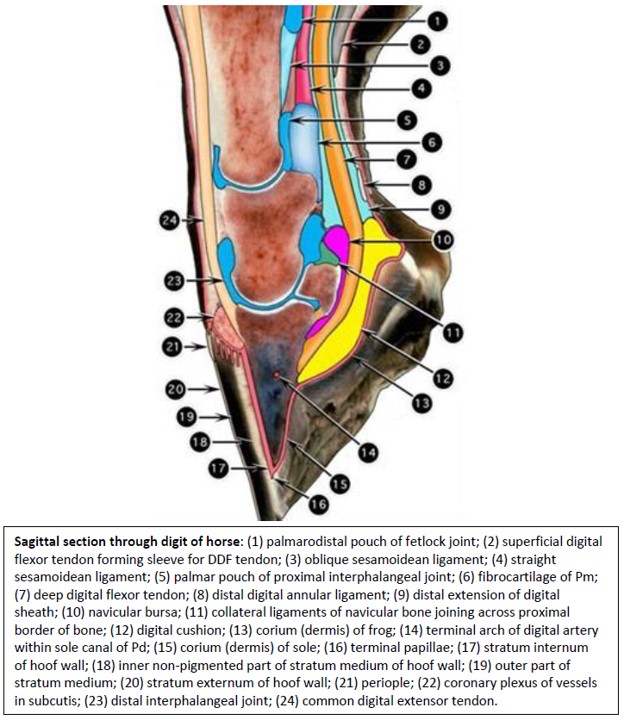
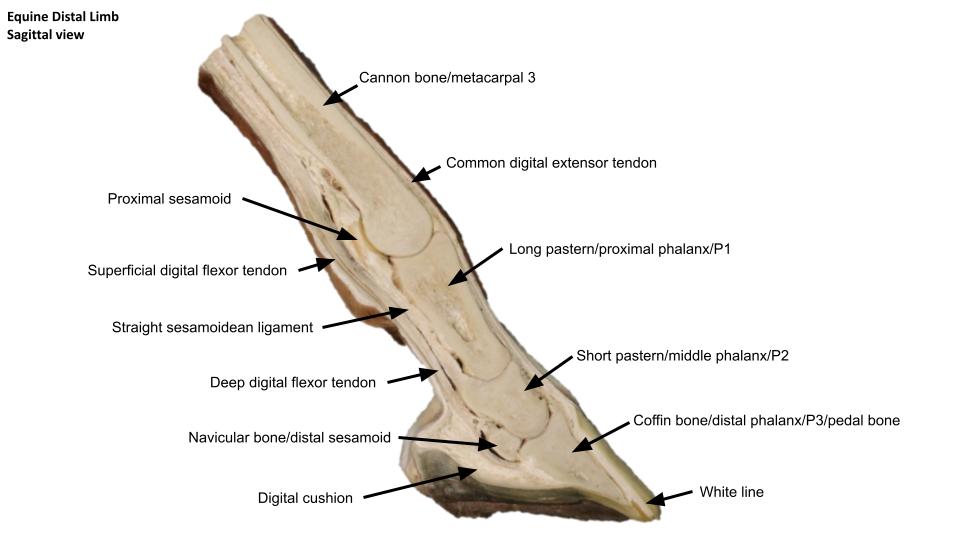
The navicular bone is anchored distally by the distal navicular ligament (commonly referred to as the impar ligament) that passes from the distal border of the navicular bone to the flexor surface of the Pd. Medial and lateral collateral (suspensory) ligaments of the navicular bone connect from its proximal border and extremities, to the Pp. Located between the DDFT and the flexor surface of the navicular bone is the navicular (podotrochlear) bursa.
Observe: Examine the navicular bone and its ligaments and bursa on prosections. Midline or sagittal sections of the distal limb show most of this anatomy very well. Note the close proximity of the digital flexor tendon sheath, the distal interphalangeal joint and the navicular bursa. Only a small, T-shaped connective tissue bridge separates them. Appendix on synovial structures.
Clinical Relevance: navicular ligaments and bursa
Transection of the collateral ligaments of the navicular bone to treat navicular syndrome; injection of the navicular bursa; navicular bursoscopy; penetrating foot injuries can enter various synovial spaces due to close proximity of structures.
-
- Equine Suspensory Apparatus and Other Ligaments; Caudomedial View. 2
-
- Palmar plantar View of the Distal Sesamoidean Ligaments of the Equine Limb. A. Superficial. B. Intermediate. C. Deep. 9
-
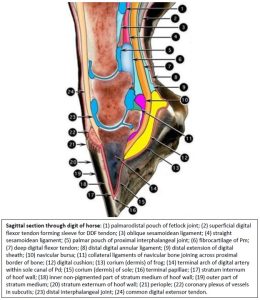
- Sagittal section through digit of horse. 2
-
- Palmaromedial aspect of the right digital area of the horse after removal of the flexor tendons. 17
-
- Palmarolateral aspect of the right digital area of the horse after removal of the flexor tendons and straight sesamoidean ligament. 17
-
- Palmar aspect of the right digital area of the horse after removal of the flexor tendons as well as straight and lateral oblique sesamoidean ligaments. 17
-
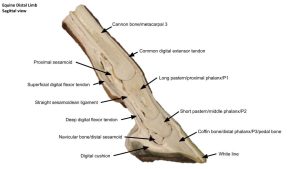
- Horse distal limb
Suspensory apparatus – horse
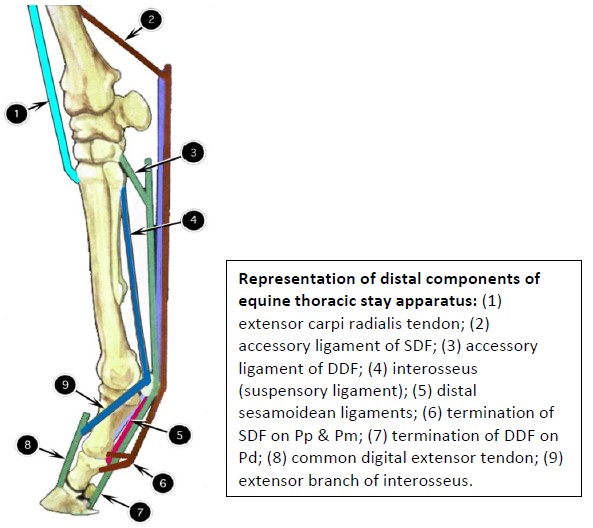
Observe: Tying together related anatomical structures, note that the 3rd interosseus m. (suspensory ligament), proximal sesamoid bones and their distal ligaments (straight, oblique, cruciate, short) form a strong, fibro-osseous support for the normal angulation of the fetlock joint. This fibro-osseous support is called the suspensory apparatus (same exists in pelvic limb).
These structures are under significant tension, even when the horse is standing still. This tension is greatly increased during athletic endeavors, which explains why these structures are vulnerable to damage during racing, jumping, and other types of athletic activity. The straight sesamoidean ligament also crosses the proximal interphalangeal joint, which it helps stabilize during weight-bearing.
In addition to the suspensory apparatus, both the DDF and SDF help support the fetlock. Because of their accessory (check) ligaments and the large amount of fibrous tissue in the muscle bellies, this support is also partly passive. Passive support is particularly important at rest and, after the muscles have fatigued, during exercise. For optional review, see the TL passive stay apparatus summary in the Appendix to tie all this anatomy together.
-
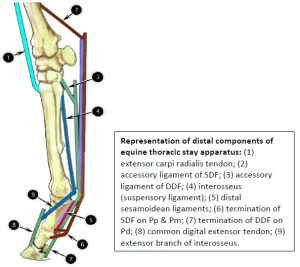
- Representation of distal components of equine thoracic stay apparatus 2
Interactive Review Content:
Ruminants
Carpal and metacarpal region
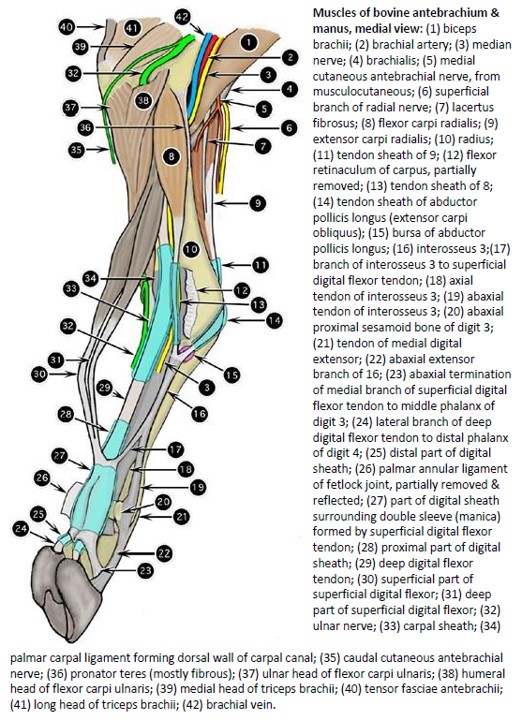
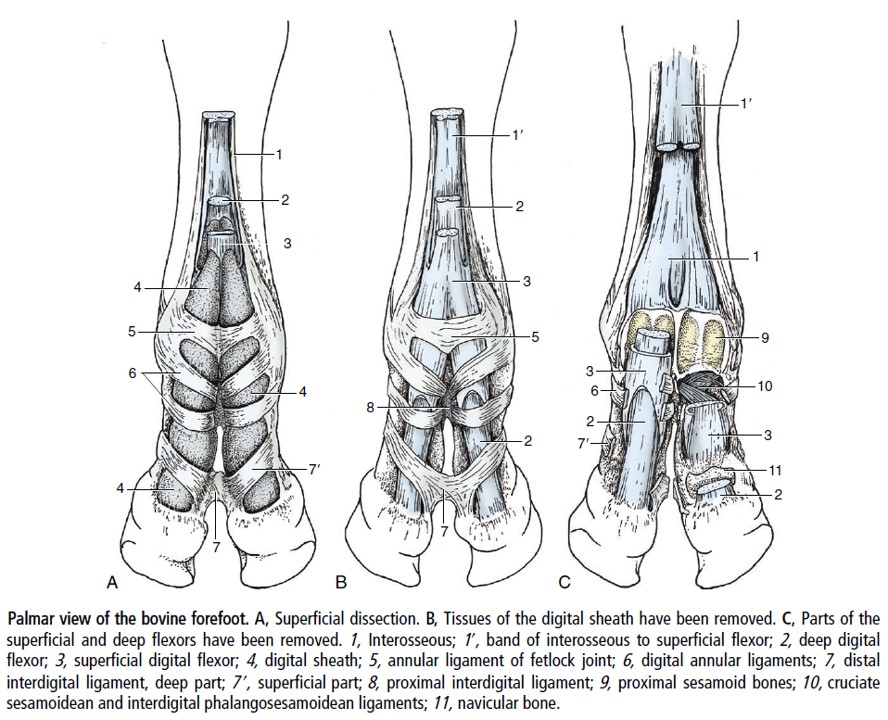
The carpal canal of the ruminant is similar to the horse in construct, with the accessory carpal bone, the palmar carpal ligament and the flexor retinaculum forming the boundaries of the canal. Notable, the flexor retinaculum in ruminants has a superficial and deep part. Recall that the superficial digital flexor m. in ruminants has superficial and deep bellies, their tendons combining in the distal metacarpal region. The deep part of the superficial digital flexor m. passes through the carpal canal in ruminants. The superficial part of the superficial digital flexor is sandwiched between the superficial and deep parts of the flexor retinaculum i.e. it lies outside of the canal.
The ruminant has two interossei mm. (3 and 4), which are fused along their axial borders. In young calves the interossei are more muscular and they become fibrous with age. In the mid-metacarpus, the interossei give off fibrous branches to the SDF tendons, which assist in the formation of the sleeves for the DDF tendons to pass through. Above the fetlock, each interosseous muscle divides into axial and abaxial tendons to insert on their respective proximal sesamoid bones for each digit. Extensor branches pass dorsally to insert into the extensor tendons of each digit (similar to horse arrangement).
Observe: review ruminant models to observe flexor tendons and the suspensory ligament (combined interossei mm. 3&4) in the metacarpal region.
-
- Muscles of bovine antebrachium & manus, medial view. 2
-
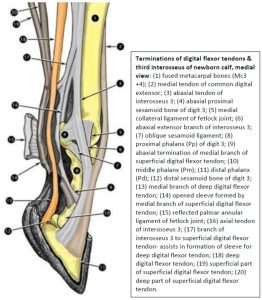
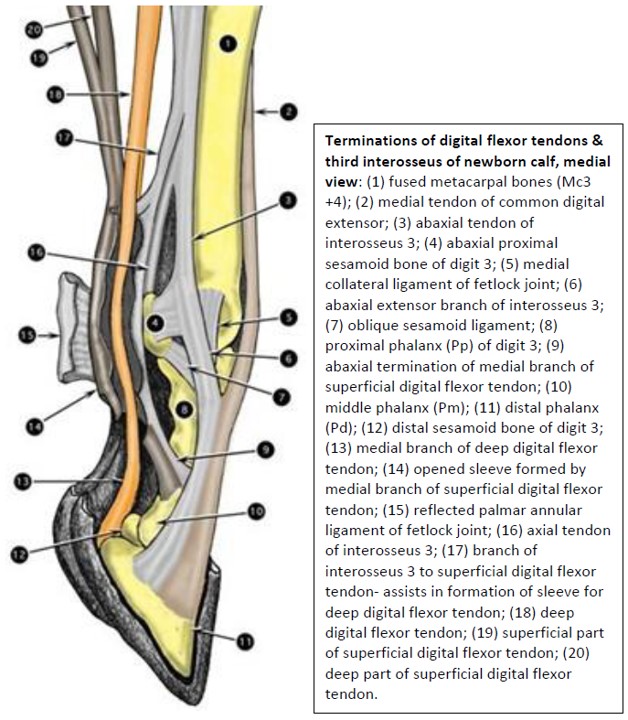
- Terminations of digital flexor tendons & third interosseus of newborn calf, medial view 2
Digital flexor tendons and digit ligaments
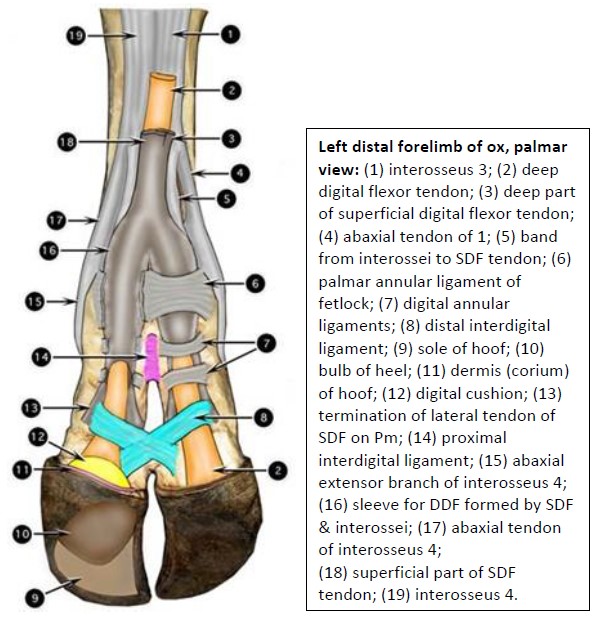
Observe: Study prosections. Note the flexor tendons bifurcate in the distal metacarpus to provide an insertion tendon for digits 3 and 4 (i.e. the medial and lateral ‘claws’). The fused 3rd and 4th interossei mm. (aka suspensory ligament) of the ruminant lie most deeply, against the palmar surface of the fused metacarpal bones III and IV. The suspensory divides and attaches similar to the horse, but does so for two digits, rather than one.
The flexor tendons are held in position on the palmar fetlock by the palmar annular ligament of the fetlock (there is one for each digit). Much like a retinaculum, the palmar annular ligament retains the tendons in the channel created by the proximal sesamoid bones.
Digital annular ligaments and manica flexorii are also present in the ruminant, a set for each digit. These need not be identified.
Two ligaments are especially clinically important in the ruminant, the proximal and distal interdigital ligaments, which should be observed on a model.
The proximal interdigital ligament is a short, thick ligament that connects the axial proximal halves of the proximal phalanges. It is present in the ox and goat, but not the sheep. The distal interdigital ligament courses between the middle phalanx of one digit and the distal sesamoid bone of the other digit, forming a cruciate structure, in the ox and goat. In the sheep the distal interdigital ligament courses transversely. The distal interdigital ligaments provides additional support by preventing spreading of the distal digits.
Observe: Identify the interdigital ligaments and the palmar annular ligament on models.
Clinical Relevance – interdigital ligaments.
In severe cases of osteomyelitis of a digit (foot rot), or a severe distal fracture, a surgical amputation of the affected digit may be performed, usually with a gigli wire saw, cutting obliquely (proximoabaxially) through the distal half of Pp. The proximal interdigital ligament is thus ideally preserved to provide important stabilizing support for the stump of the amputated digit. The distal interdigital ligament however must be transected to allow removal of the amputated digit.
-

- Left distal forelimb of ox, palmar view 2
-
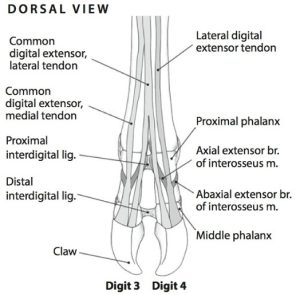
- Left digits of the ox, dorsal view. 6
-
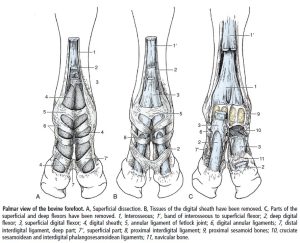
- Palmar view of the cow forefoot. 8
-
- Terminations of digital flexor tendons & third interosseus of newborn calf, medial view 2
Clinical Application: Q5
 Review the image and ponder the following questions.
Review the image and ponder the following questions.
1) What common cutting device is being used to amputate the digit (claw)?
2) What ligament of the ruminant foot must be transected to allow removal of one digit, if amputation is through the mid shaft of the proximal phalanx?
3) Note the green butterfly catheter and orange torniquet (mid left in image) – what vessel has likely been catheterized? What drug may have been injected? These questions are for general curiosity at this time. Vessels will covered in the cardiovascular system.
(Answer)
Interactive Review Content:
Lab 7 Appendix
FYI only – Passive stay apparatus of equine thoracic limb
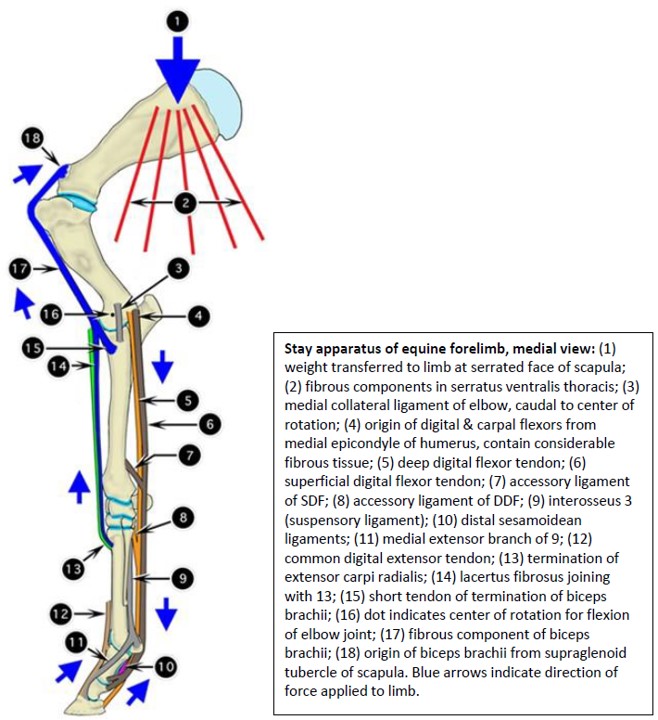
In contrast to the pelvic limb, in which everything centers around locking the patella of one limb and involves shifting the support alternately between limbs, the stay apparatus of the thoracic limbs functions concurrently. When standing squarely, horses support more weight on their thoracic limbs, largely because the head and neck are heavy, and their forward overhang moves the center of gravity of the horse to a level about 38 cm (~16 inches) caudal to the tuber olecrani.
Body weight is transferred to the forelimb primarily at the serrated face of the scapula by way of the attachment of the serratus ventralis. The thoracic part of the serratus ventralis has a thick epimysium, and the muscle itself contains considerable connective tissue, making the transfer largely passive. This point of weight transfer is caudal to the shoulder joint. Flexion (collapse) of the shoulder is prevented by the fibrous band of the biceps, supplemented by a fibrocartilaginous mold over the intermediate tuberosity of the intertubercular groove. Continuation of this fibrous band through the lacertus fibrosus and the extensor carpi radialis tendon pulls a tight, stabilizing band across the dorsum of the carpus, which helps the horse resist buckling forward into flexion.
The digital flexor tendons, with their accessory ligaments, are pulled tightly across the palmar surface of the carpus and provide additional resistance to flexion of this joint complex. As these tendons continue around the fetlock, they help form a fibrous sling for this joint to fall back into. Importantly, the fibro-osseous sling provided by the suspensory apparatus (suspensory ligament, proximal sesamoid bones and the [distal] sesamoidean ligaments) provides great support for the fetlock. The weight-induced traction provided by the extensor branches of the suspensory ligament connecting to the CDE, which inserts on the extensor process of Pd, offsets the flexion pull on the DIPJ produced by the DDF tension.
The only joint subject to question is the elbow. Although the triceps brachii muscle is necessary to set the elbow in its weight- bearing position, it does not appear to do much once everything is set (palpate the “soft” triceps brachii m. in the standing horse). Initial flexion of the elbow joint in the weight-supporting limb is resisted by the following: (1) the digital and carpal flexor muscles, which contain much fibrous tissue, originate primarily from the medial epicondyle of the humerus and thus resist flexion by pulling down on the lever provided by the epicondyle; and (2) the collateral ligaments of the elbow, which pass caudal to the center of rotation of the joint. Thus, initial flexion of the joint is resisted because, at the onset of flexion, these ligaments must be stretched a little as their proximal attachments rotate up and over the center of rotation.
Review Videos
Terms
The below is a list of terms to confirm identification and understanding of for this lab. Note, a number of these terms have been introduced in previous labs.
| Structure/feature | Comments/species specific |
| Ligament of ergot | Horse – if remains visible after skin reflection |
| Lateral and medial collateral ligaments of carpus | |
| Carpal canal | Bound by 3 structures |
| Flexor retinaculum | |
| Palmar carpal ligament | |
| Accessory carpal bone | |
| Carpal sheath | Synovial sheath wrapped around flexor tendons in carpal canal. |
| Dorsal metacarpal ligament | Horse |
| Common digital extensor tendon(s) | Two tendons present in ruminant |
| Lateral digital extensor tendon | |
| Tendon sheath | |
| Suspensory ligament | 3rd interosseus m. in horse, fused 3rd and 4th interossei in ruminant. |
| Superficial digital flexor tendon | Two tendons in ruminant |
| Deep digital flexor tendon | |
| Accessory ligament of DDFT = distal check ligament | Horse |
| Dorsal pouch fetlock joint | Horse |
| Synovial fold | Horse – within dorsal pouch of fetlock joint |
| Palmar pouch of fetlock joint | Horse |
| Digital flexor tendon sheath | Horse |
| Manica flexoria | Horse – part of SDFT surrounding DDFT |
| Palmar (inter)sesamoidean ligament | Horse |
| Palmar annular ligament | |
| Proximal digital annular ligament | Horse |
| Distal digital annular ligament | Horse |
| Straight sesamoidean ligament | Horse |
| Oblique sesamoidean ligament | Horse |
| Cruciate sesamoidean ligament | Horse |
| Short sesamoidean ligament | Horse |
| Distal navicular ligament = impar ligament | Horse |
| Collateral (suspensory) ligaments of navicular bone | Horse |
| Navicular bursa | Horse |
| Proximal interdigital ligament | Ox |
| Distal interdigital ligament | Ox |