
MSK LAB 13A – Thoracic wall osteology, arthrology and myology
Part 1: Thoracic wall osteology and arthrology
Learning Objectives
- Describe and identify the comparative osteology of the thorax, including reference to the number of thoracic vertebrae, ribs, and sternebrae present in the canine, feline, equine, ruminant and porcine
- Identify articulations of the thoracic wall
- Identify the costal arch, thoracic inlet, thoracic outlet
- Describe the anatomy of thoracocentesis
Lab introduction:
For this 2 part lab we will first consider the bones and joints that define the skeletal thoracic wall of the thorax. In Part 2 we will dissect and explore the muscles of the thoracic wall.
The bony thoracic wall consists of thoracic vertebrae dorsally, ribs on left and right sides, and the sternum ventrally. There is an ‘inlet’ and an ‘outlet’ to the thoracic cavity. There is considerable variation in the number of vertebrae and ribs between the species we are studying, whereas the number of sternebrae are in the 6-8 range. The vertebrae have already been considered in Section 2 Lab 9A, and we will revisit here for completeness.
Observe: Refer to articulated skeletons and individual bones to examine and learn thoracic wall osteology and arthrology.
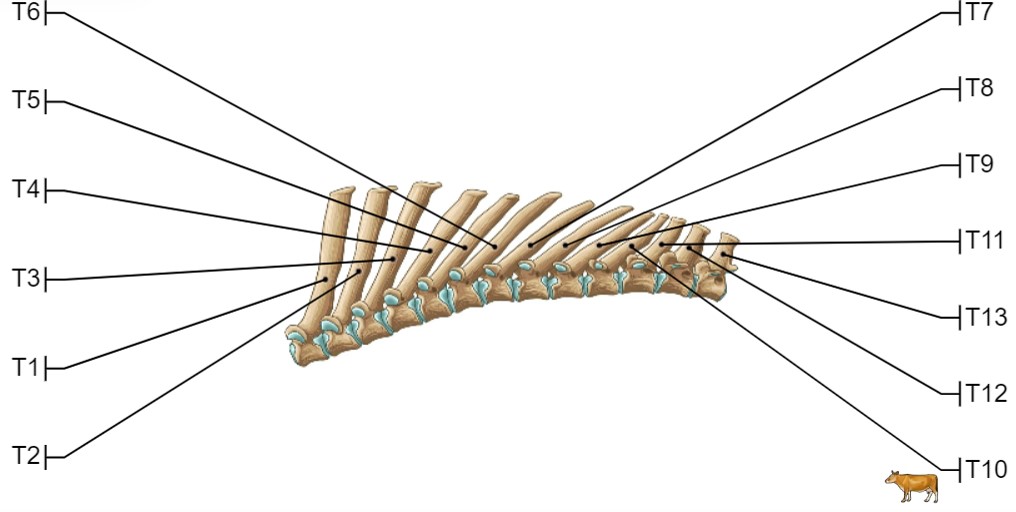
Thoracic vertebrae – comparative
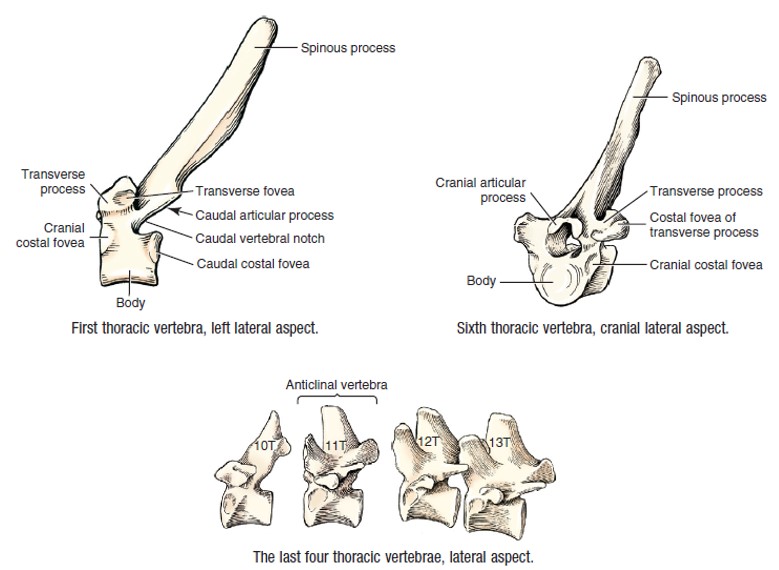
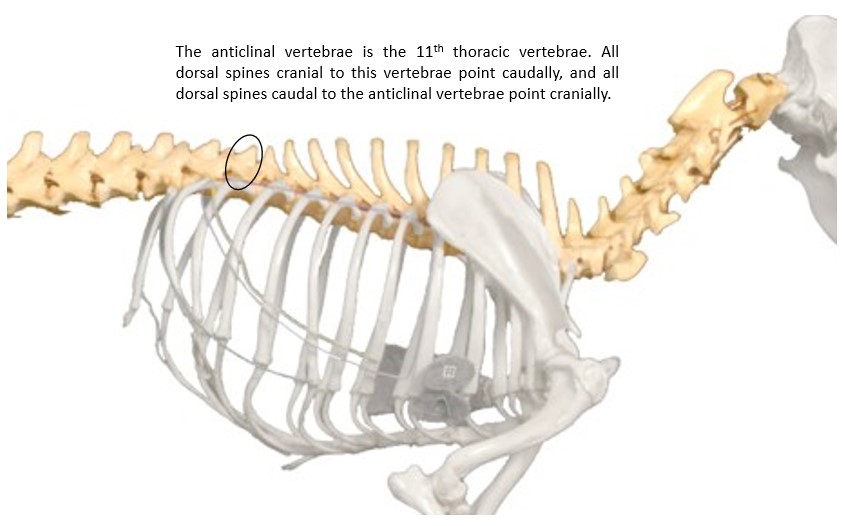
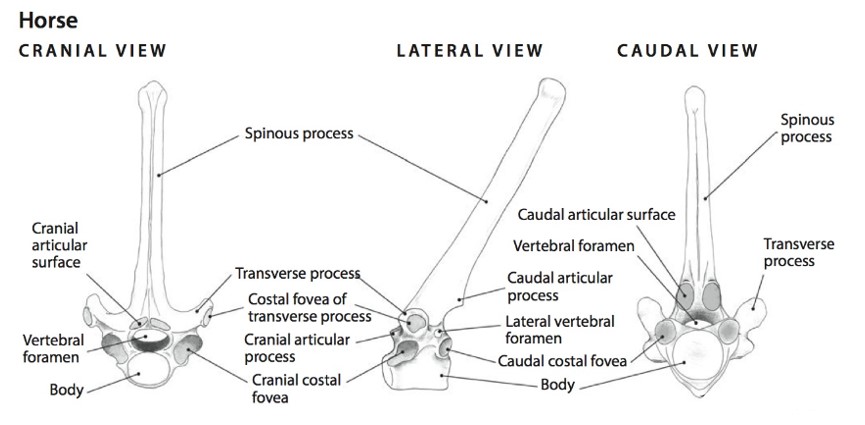
Recall from Section 2, that carnivores have 13 thoracic vertebrae, and ruminants do too. Horses, with their long, barrel-shaped thorax, typically have 18 (17-19 range) thoracic vertebrae, and pigs, 14-15. Thoracic vertebrae have a prominent spinous process, a body, an arch (consists of two pedicles and a lamina), cranial and caudal articular processes, and transverse processes. The thoracic vertebrae are also modified for articulation with the ribs. Sites where ribs join to a vertebra are identified as shallow depressions in the vertebra called costal fovea (costa [L] = rib; fovea [L] = pit, small depression). More details under the “Rib” heading. Recall that the 11th thoracic vertebra is the anticlinal vertebra in the canine.
-
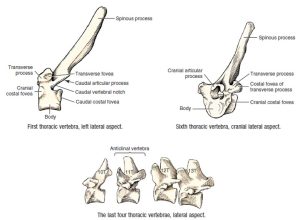
- Dog thoracic vertebrae. 3
-
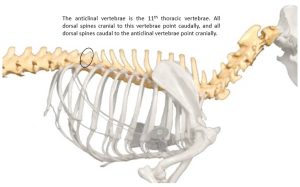
- Anticlinal vertebrae
-
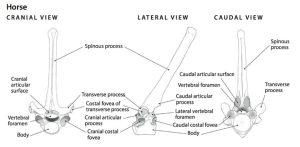
- A cranial thoracic vertebra of the horse; cranial, lateral, and caudal views. 5
-
-
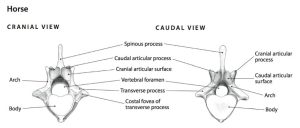
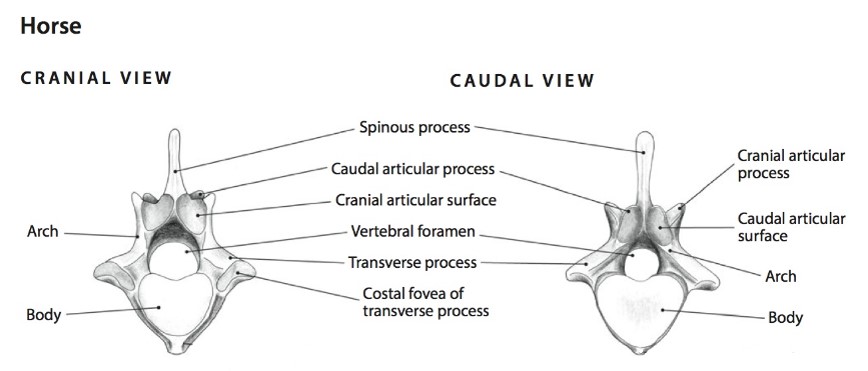
A caudal thoracic vertebra of the horse, cranial and caudal views.
5
-
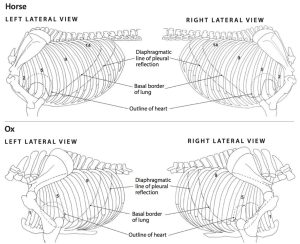
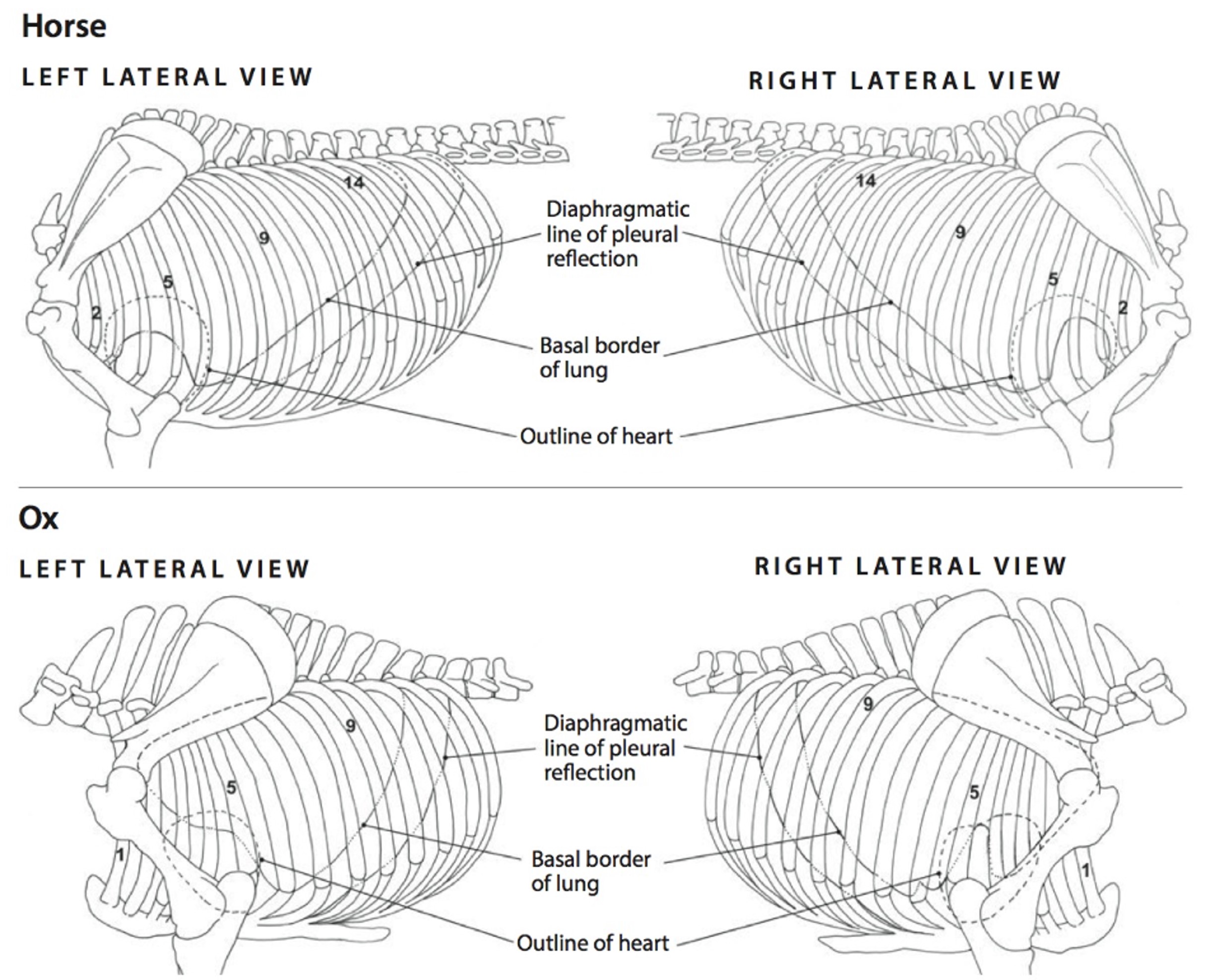
- Left and right lateral views of the thorax, lungs, and extent of pleurae in the horse and ox. 5
-
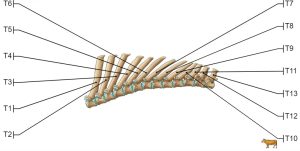
- Cow thoracic vertebrae 24
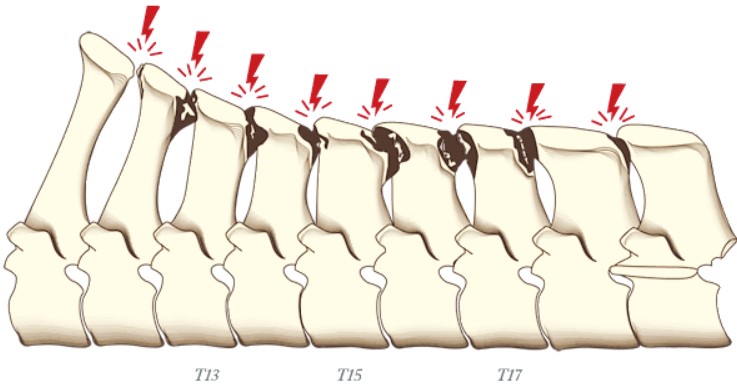
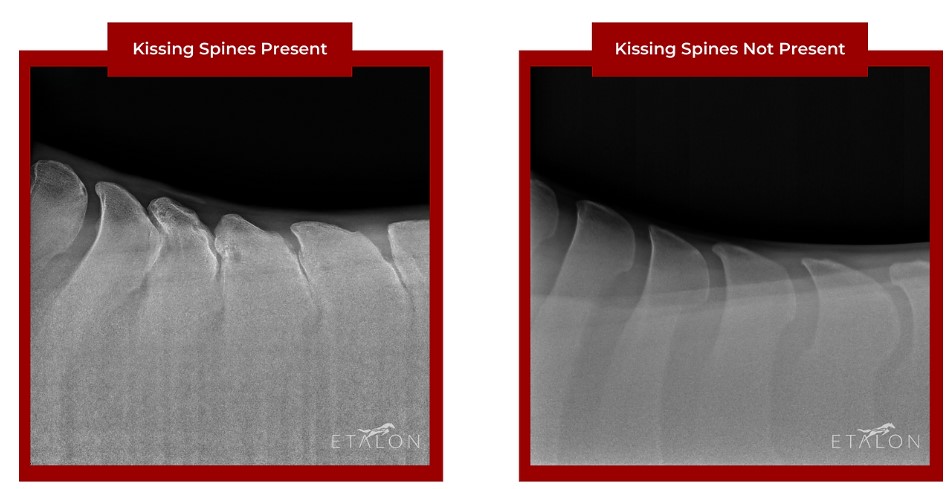
Clinical relevance: kissing spines
-
- Kissing Spine Ben Calvert
-
- Kissing spine radiograph Etalon
Ribs – comparative
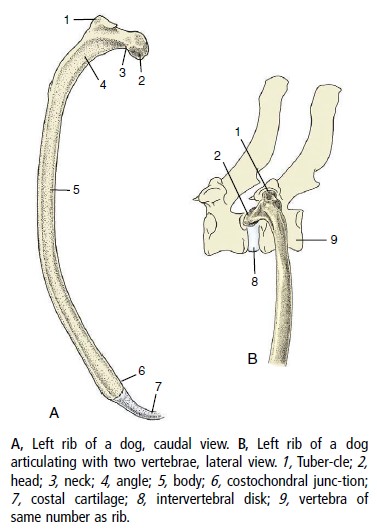
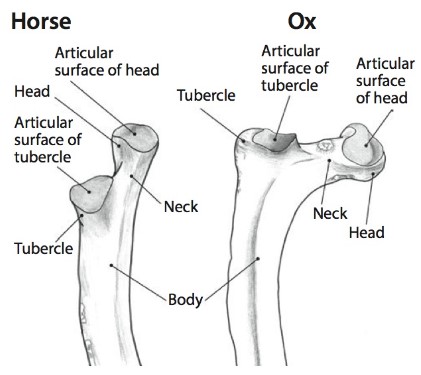
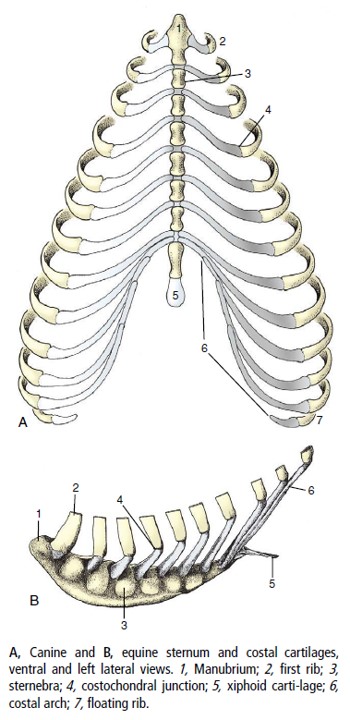
The number of rib pairs matches the number of thoracic vertebrae! The majority of the rib is bone, with features including a head, neck, tubercle, and body. Ventrally, the rib continues as a cartilaginous structure, the costal cartilage. The costochondral junction refers to the junction between osseous and cartilaginous rib. This junction may be expanded in rapidly growing animals. Costal cartilages of sternal ribs articulate directly with the sternum (8-9 pairs). The remaining caudally-located rib pairs (asternal ribs) articulate with each other via their costal cartilages. The continuous line of united costal cartilages forms the costal arch, which also represents the caudal margin of the thorax. The thirteenth pair of ribs in carnivores often end freely in the flank (‘floating’ ribs) rather than being integrated into the costal arch. Horses and ruminants do not usually have floating ribs. The space between adjacent ribs, filled with muscles, neurovascular and other soft tissues, is called the intercostal space (ICS).
FYI – In carnivores, the head of ribs 1 through 10 articulates with the cranial and caudal costal foveae of adjacent vertebrae and with the associated intervertebral disk. For ribs 11 through 13, the head articulates only with the cranial costal fovea on the body of the vertebra of the same number. The tubercle of the rib articulates with the costal fovea of the transverse process of the vertebra of the same number. In ungulates, the rib head of all ribs articulates with cranial and caudal costal fovea of adjacent vertebrae, and with the associated intervertebral disk. The tubercle articulation is the same as carnivores.
Clinical relevance: fractures, tumors, access to the thoracic cavity
-
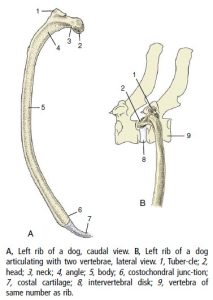
- Dog ribs. 8
-
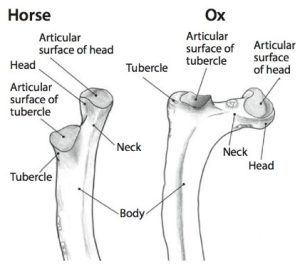
- Proximal portion of a rib of the horse and ox. 5
-
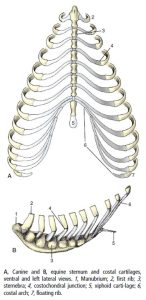
- Canine and equine sternum and costal cartilages. 8
Sternum – comparative
The sternum is composed of a column of bony segments, the sternebrae (singular, sternebra) united by intervening cartilages, or sometimes fused together. Carnivores have eight (8) sternebrae, the horse and ruminant seven (7), and the pig, six (6). The first sternebra, also known as the manubrium, ends cranially in a clublike enlargement. The last sternebra is flattened dorsoventrally and is called the xiphoid process. The caudal end of this process is continued by a thin plate, the xiphoid cartilage.
Clinical relevance: bone marrow source; palpable landmarks for procedures; sternotomy to access the thoracic cavity.
Clinical application: Q1
Q1. Harvesting of bone marrow is performed for the cultivation of bone marrow-derived multipotent mesenchymal stromal cells (BM-MSCs) used in regenerative therapies. The sternum is often a harvest site. How many sternebrae are present in the ruminant and horse?
Thoracic inlet and outlet
The thoracic cavity is bound primarily by bone, cartilage and muscle. Cranial, caudal, dorsal, ventral and lateral boundaries exist. The cranial boundary is termed the thoracic inlet, defined by the manubrium (first sternebra), the pair of first ribs and the first thoracic vertebra (T1). Neck viscera pass through the thoracic inlet to enter the thoracic cavity. The caudal boundary is defined as the thoracic outlet. The thoracic outlet is bound by the last thoracic vertebra dorsally, the last rib pair and the costal arches laterally, the xiphoid process ventrally (i.e. the most caudal sternabra), and the diaphragm (to be studied in a future unit). The dorsal boundary is formed primarily by the thoracic vertebrae, along with epaxial and hypaxial muscles associated with this part of the vertebral column. The pairs of ribs and their costal cartilages and intercostal mm. form the lateral boundaries. The sternum and ventral thoracic mm. (rectus thoracis m. and transversus thoracis m. – see myology lab) form the ventral boundary.
Thoracocentesis (thoracentesis, chest tap)
Thoraco-(from Thorax [Gk] – chest) and centesis (from Kentesis [Gk] – a pricking, puncturing) means to pass a device (e.g. a needle, catheter, chest tube) through the thoracic wall, into the thoracic cavity (specifically, the pleural cavity, and pleurocentesis or pleural tap is occasionally used). It is an important clinical procedure involving the thoracic wall anatomy. The pleural cavity will be defined in detail in the Respiratory System unit. For now, understand it to be a space, that normally is ’empty’ and in disease states it can fill with air or fluid (or a mass). Clinically we need to remove this air or fluid and to access the pleural cavity we may perform a thoracocentesis. Often this is done under emergency conditions to alleviate respiratory distress. We want to be caudal to the heart and still access the more cranioventral pleural cavity for optimal fluid removal. For air removal we may be more caudal and dorsal (particularly in a standing animal, as is common in large animal thoracocentesis). In small animals, low stress restraint, in sternal recumbency or standing, if possible, is also ideal for the already distressed animal.
The general rule of thumb, across small and large animals, for the anatomical approach for thoracocentesis to drain fluid is:
- 7th-8th ICS; on a level about halfway between elbow and shoulder joints i.e. just above the costochondral junction; on the cranial margin of the rib!
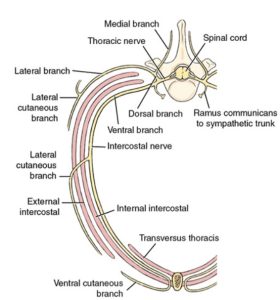
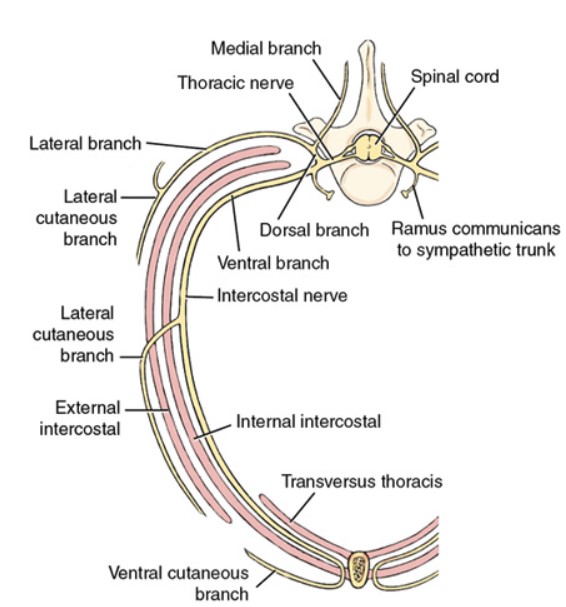
Why the cranial margin of the rib? Because on the caudal margin there are vessels and a nerve passing along the rib surface and we wish to avoid injuring these structures (these structures will be visited in future units).
Clinical relevance: thoracocentesis
Thoracocentesis is often an emergency procedure to restore respiratory function e.g. in the case of acute pneumothorax (air that has accumulated in the pleural cavity causing lung collapse). Accumulated fluid in the pleural cavity is sampled, and drained, via thoracocentesis.

Terms
| Thorax osteology and arthrology |
|
| Thoracic vertebrae |
Canine 13, Ruminant 13, Pig 14-15, Horse 18 |
| (Dorsal) spinous process | |
| transverse process | |
| cranial/caudal articular processes | |
| body | |
| arch (consisting of two pedicles and the lamina) | |
| costal fovea | |
| anticlinal vertebra (T11) in canine | |
| Ribs – paired. Same number as thoracic vertebrae | Head |
| Neck | |
| Tubercle | |
| Body | |
| Costochondral junction | |
| Costal cartilage | |
| Costal arch | |
| Intercostal space | |
| Sternum – sternebrae and number |
carnivore 8, horse and ruminant 7, pig 6 |
| Manubrium | |
| Xiphoid process and xiphoid cartilage | |
| Thoracic inlet | define boundaries |
| Thoracic outlet | define boundaries |
| Thoracocentesis |
define typical location as described |
Part 2 – Thoracic wall muscles
Learning Objectives
- Identify the muscles of the lateral thoracic walls (including the serratus dorsalis mm. again)
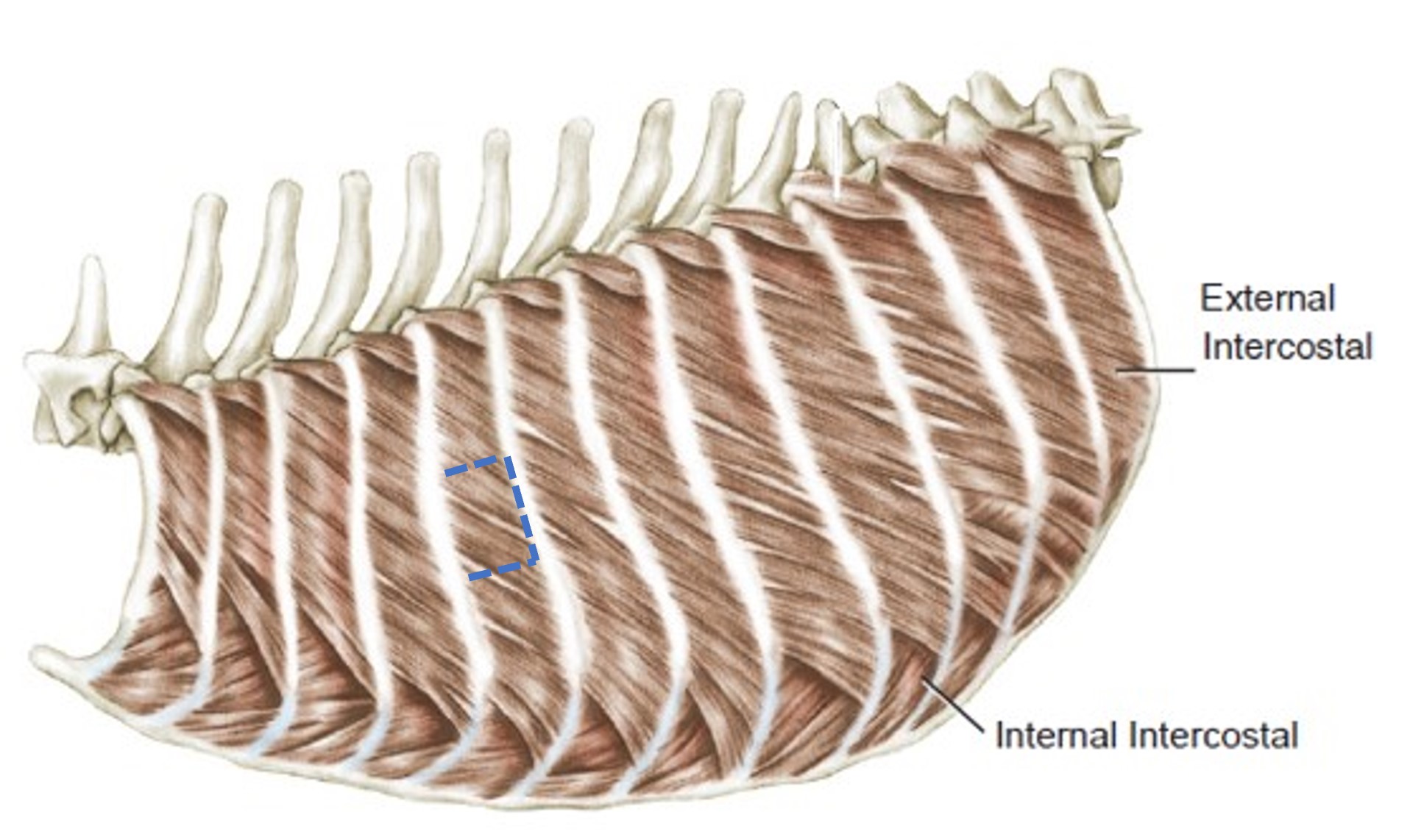
- Recognize that the muscle fiber directions of the external and internal intercostal mm. run perpendicular to each other.
Part 2 lab instructions:
Building on the skeletal anatomy of the thoracic wall, we will now dissect and identify thoracic wall muscles. Examination of prosected large animal cadavers and available lab specimens (wet and dry) is also required.
Read the following descriptions of muscles and perform dissection as directed. All dissection is continued on the left side of the cadaver. Refer to ungulate prosected cadavers for the comparative anatomy as instructed.
The serratus ventralis mm. (cervicis and thoracis parts) have been studied with the thoracic limb and are not considered further here.
Dissect: Following the amputation of the left thoracic limb, and during the dissection of epaxial muscles, stumps of serratus ventralis m. may remain – excise any remaining portions of the serratus ventralis m. from the left thoracic wall and discard.
Serratus dorsalis m.
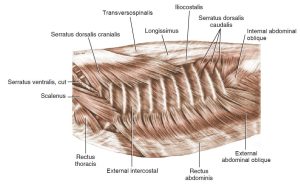
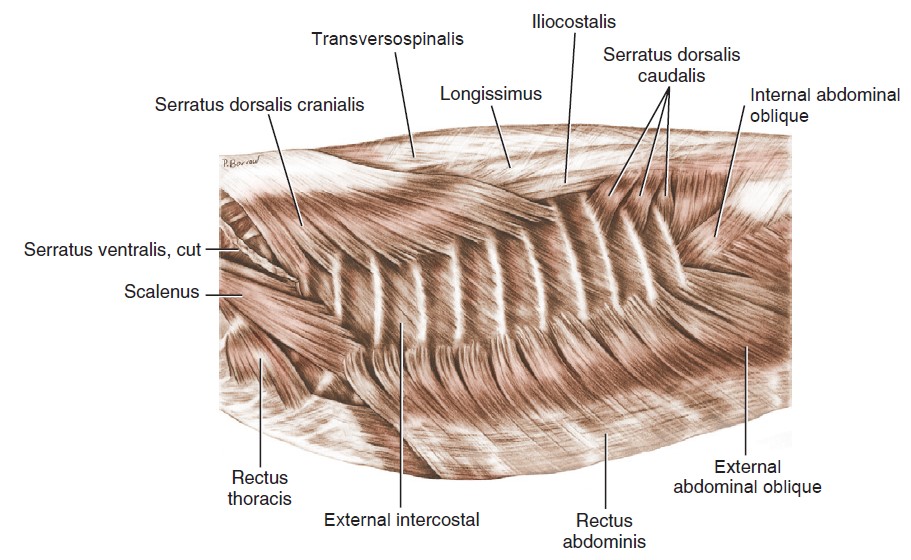
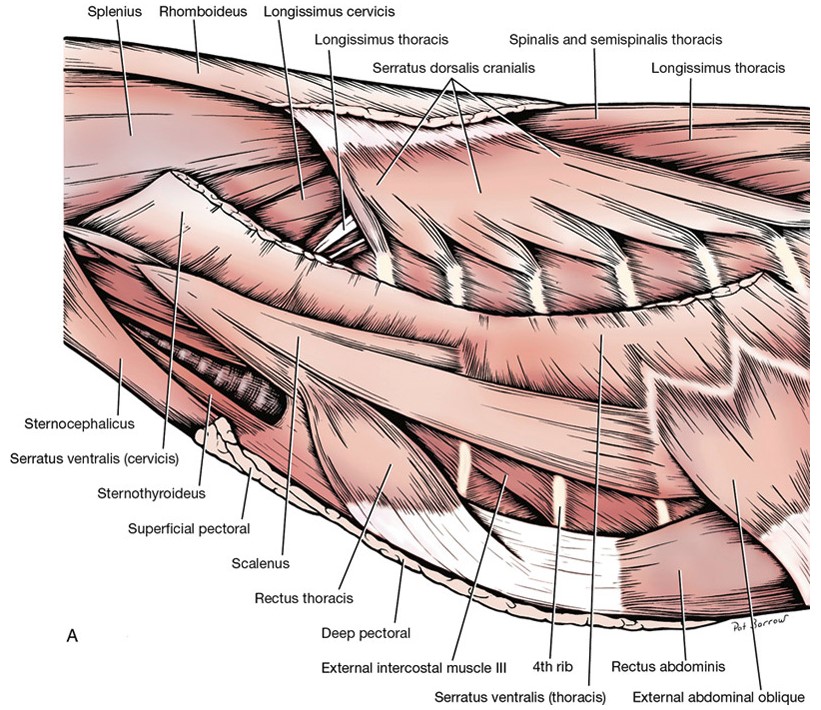
The serratus dorsalis m. consists of cranial and caudal divisions. The serratus dorsalis cranialis m. lies on the dorsal surface of the cranial thorax. It arises by a broad aponeurosis from the thoracolumbar fascia deep to the rhomboideus m. It runs caudoventrally and inserts by distinct serrations on the craniolateral surfaces of the ribs. It lifts the ribs for inspiration. The serratus dorsalis caudalis m. is smaller and is found on the dorsal surface of the caudal thorax. It consists of (in)distinct muscle leaves that arise by an aponeurosis from the thoracolumbar fascia, course cranioventrally, and insert on the caudal borders of the last three ribs. It functions in drawing the last three ribs caudally in expiration.
Dissect: Identify the serratus dorsalis mm., elevated during the epaxial mm. dissection.
-
- Superficial muscles of thoracic cage, lateral aspect. 3
-
- Superficial musculature of the neck and thorax of the cat with thoracic limb removed, lateral view. 4
-

- Dog thoracic wall
Scalenus m.
The scalenus m. lies ventral to the origin of the cervical and thoracic parts of the serratus ventralis m. It attaches to the first few ribs and the transverse processes of the cervical vertebrae and is divided into several slips. It is a muscle of inspiration, pulling the cranial ribs cranially and anchoring them. Branches of cervical spinal nerves (C5-C7 range) pass over the surface of the scalenus m. before they unite to form the phrenic n. at about the first rib. (What muscle does the phrenic nerve innervate? This nerve will be considered in detail in the Nervous and Respiratory Systems).
Dissect: Identify the scalenus m. as it remains after thoracic limb removal. It may be quite disrupted.
-
- Superficial muscles of thoracic cage, lateral aspect. 3
-
- Superficial musculature of the neck and thorax of the cat with thoracic limb removed, lateral view. 4
-
- Dog thoracic wall
-
- Dog scalenus. 40
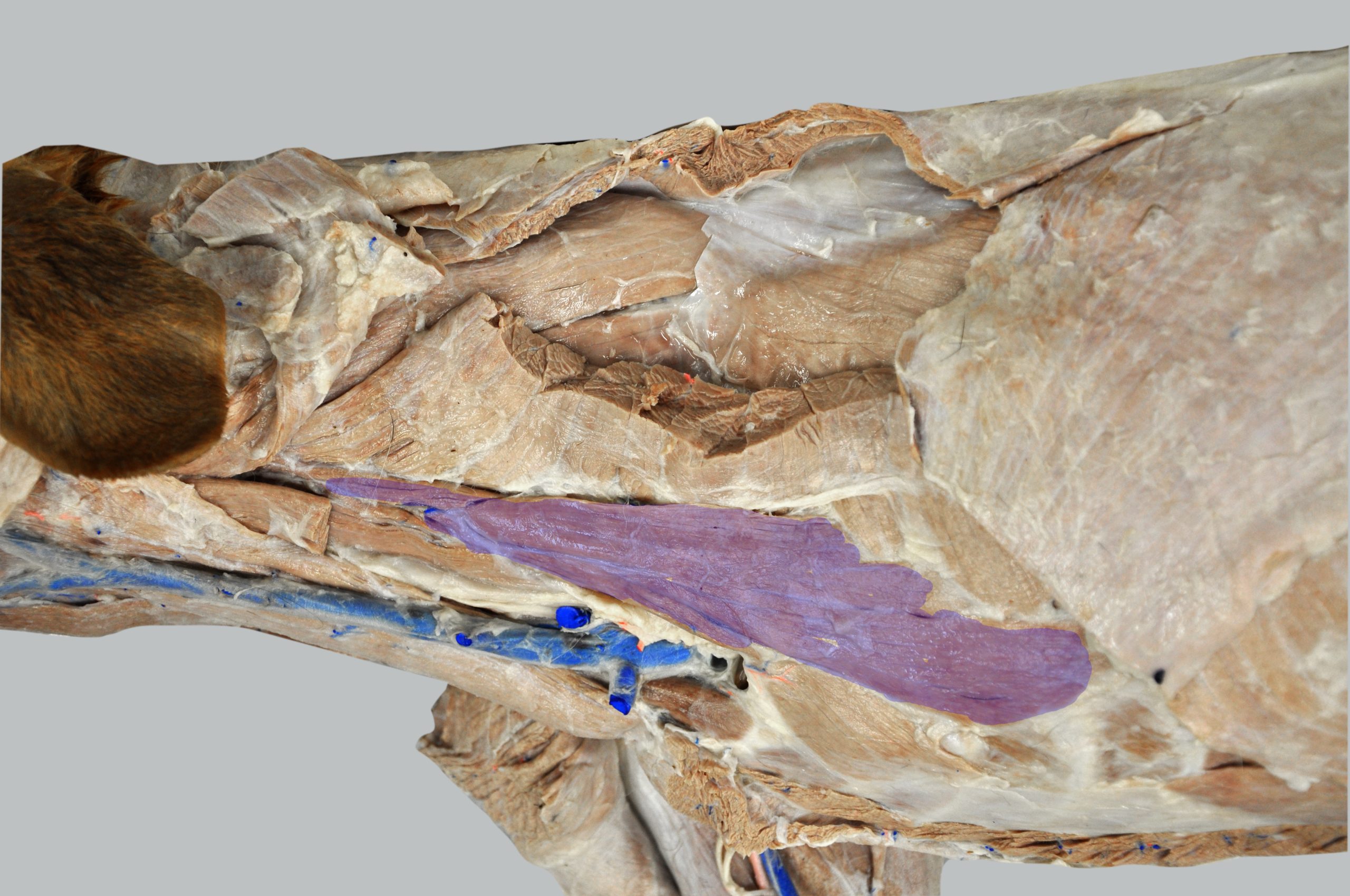
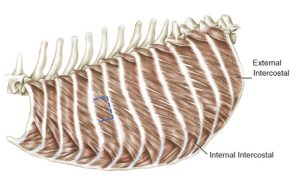
Intercostal muscles
There are 12 external intercostal mm. on each side of the thoracic wall. Their fibers run caudoventrally in the intercostal space, from the caudal border of one rib to the cranial border of the rib caudal to it. The external intercostal mm. extend ventrally, but only to the level of the costochondral junction. They function in respiration by drawing the ribs together.
The internal intercostal mm., the next muscle layer deep to the external intercostal mm., are easily differentiated from the external intercostal mm. because their fibers run cranioventrally from the cranial border of one rib to the caudal border of the rib cranial to it. Then, layered on the deep side of the internal intercostal mm. is endothoracic fascia, which in turn is lined by a serous membrane called pleura (reviewed in the Respiratory System unit). The internal intercostal mm. occupy the entire intercostal space, from dorsal to ventral, i.e. they continue to the sternum. These muscles function similar to that of the external intercostal mm., by drawing the ribs together.
Dissect: Remove fascia as needed to clearly view the external intercostal muscles at the mid thorax level. Count intercostal spaces to identify the fifth external intercostal muscle; carefully cut a 3-sided ‘window’ in this muscle and reflect it to observe the underlying internal intercostal m. These muscles are thin and finding the fascial plane between them requires gentle dissection. It may take a few attempts.
-
- Deep muscles of thorax, lateral aspect. 1
Rectus thoracis m.
The rectus thoracis m. is a thin slip of muscle that extends from the ventrolateral sternum cranially and obliquely to insert on the first rib. It has a role in inspiration. This muscle is the thoracic wall continuation of the much more developed rectus abdominus (‘6 pack’) muscle of the ventral abdominal wall (to be considered in the next lab).
Dissect: The rectus thoracis m. lies ventral to the scalenus m. Clear away fascia as needed to identify the muscle.
-
- Muscles of neck and thorax, lateral view. 1
Transversus thoracis m.
The transversus thoracis m. lines the internal ventral thoracic cavity on the left and right sides, extending from the sternum laterally to the costochondral junction level. The muscle is visible in an opened thoracic cavity (to be performed in a later unit). This muscle assists with expiration.
Observe: Identify the transversus thoracis m. on the available plastinated specimens in the lab. We will view this muscle on cadavers after the thoracic cavity is opened.
-
- Muscles of the thoracic wall of the dog. 1
-
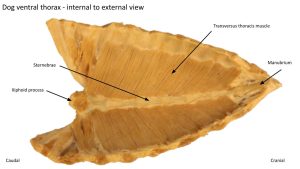
- Transversus thoracis.
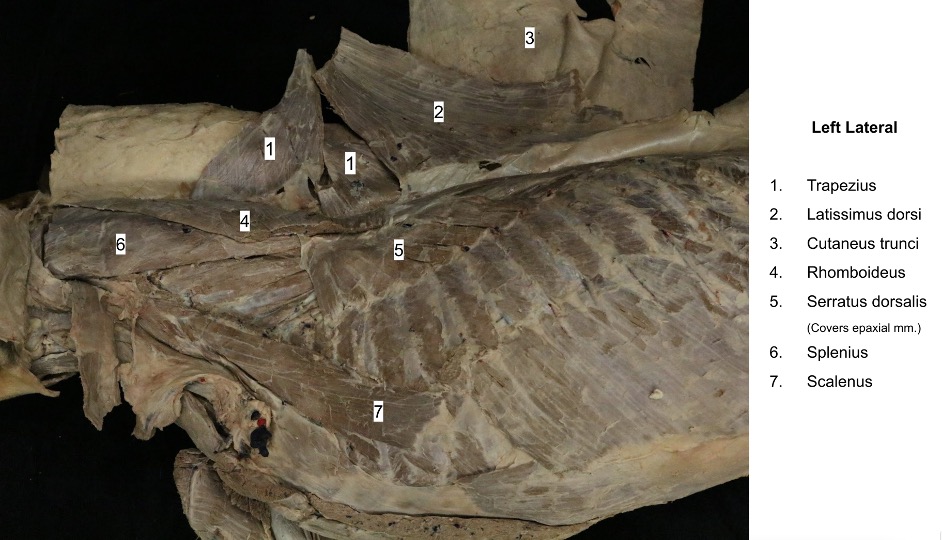
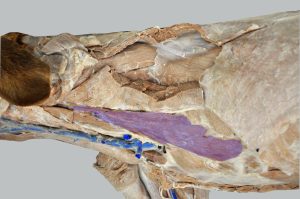
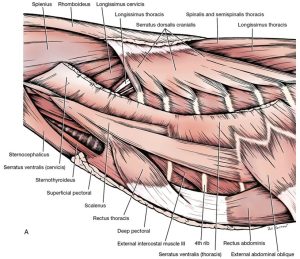
Ungulate comparative thoracic wall myology
Observe: Examine prosected cadavers to study the comparative thoracic wall myology. Identify the serratus dorsalis, scalenus, rectus thoracis, and external and internal intercostal mm. Phrenic nerve roots from C5-C7 spinal nerves, crossing the ventral scalenus m., are easier to see in the large animal. Ungulates have multiple bellies to the scalenus m.
Clinical relevance: depth of thoracic wall incisions or traumatic wounds
Clinical relevance: phrenic n.
-
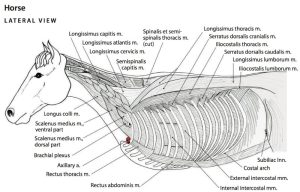
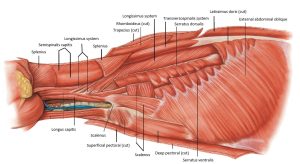
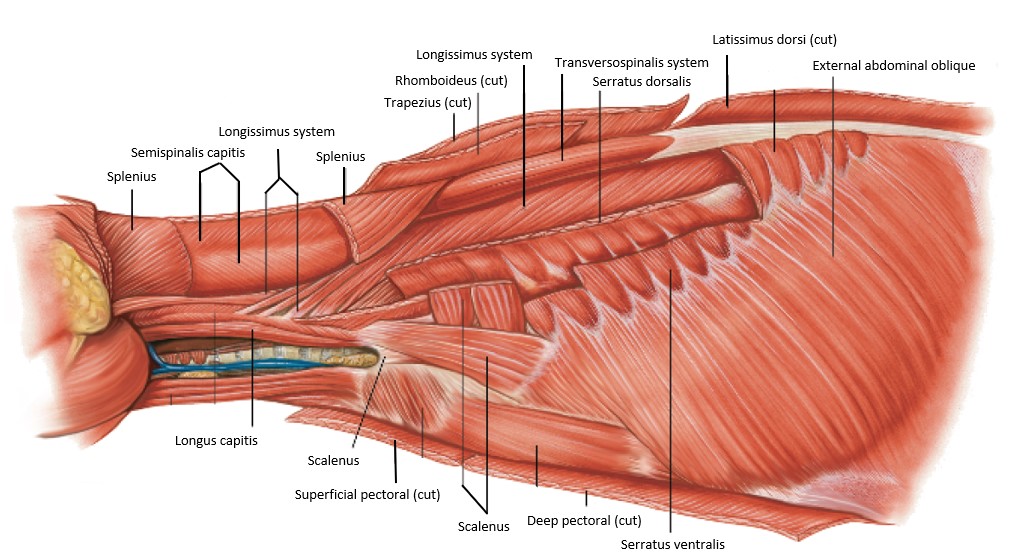
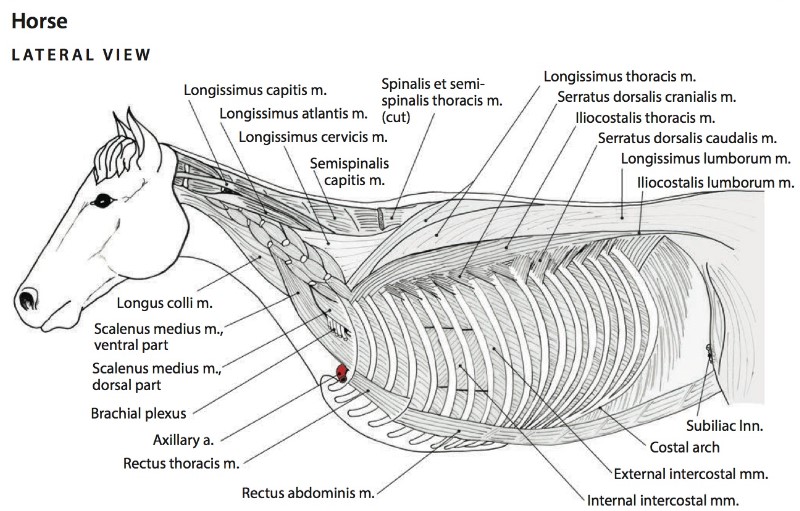
- Thoracic wall and select axial muscles of the horse. The thoracic limb and serratus ventralis thoracis muscle have been removed. 6
-
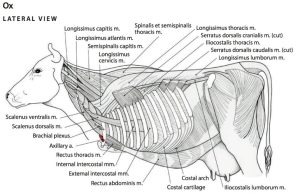
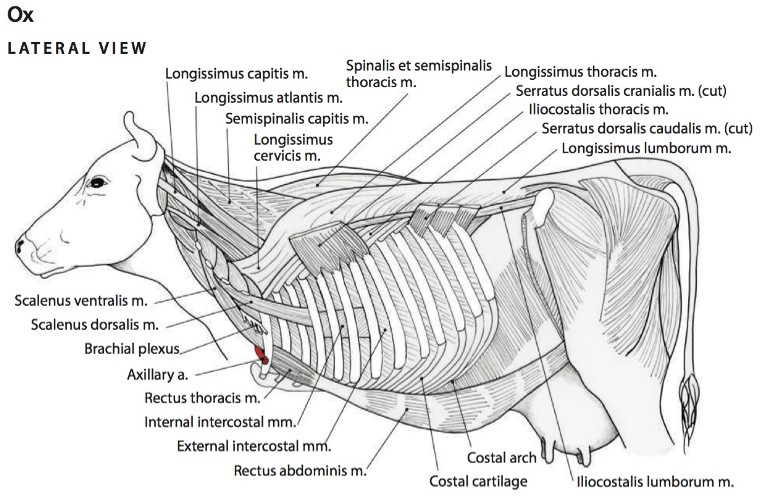
- Thoracic wall and select axial muscles of the ox. The thoracic limb and serratus ventralis thoracis muscle have been removed. 6
-
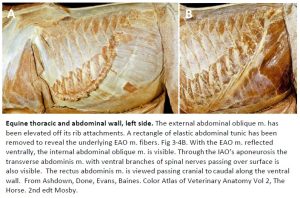
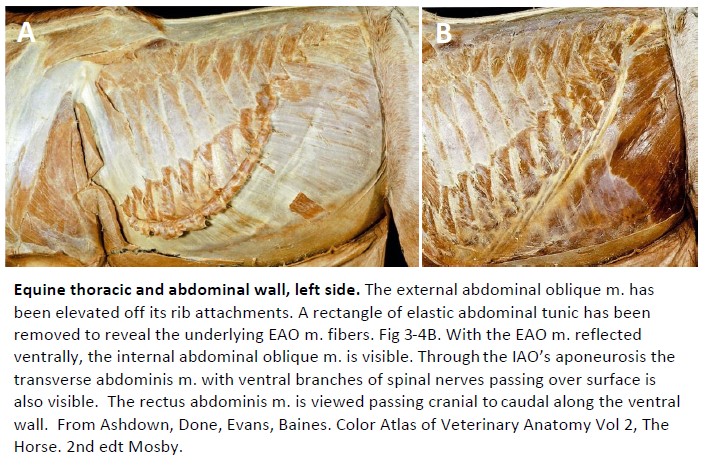
- Equine thoracic and abdominal wall, left side. 15
Review Videos
Ungulate thoracic osteology – 5 min
Terms
| Thoracic wall myology and comments |
|
| Serratus dorsalis mm. | cranial and caudal divisions |
| Scalenus m. | multiple slips or divisions |
| External intercostal mm. | |
| Internal intercostal mm. | |
| Rectus thoracis m. | |
| Transversus thoracis m. | Learn on a model at this time |