Lab 2: Thoracic Vasculature and Lymphatics
Learning Outcomes
- Identify the vessels and nerves of the thoracic wall.
- Describe the location of the intercostal aa, vv, and nn (the neuromuscular bundle) relative to each rib/intercostal space, and the clinical importance of this information.
- Name and identify the great vessels of the heart and their branches.
- Name and identify the branches of the thoracic part of the descending aorta.
- Identify and describe the afferent and efferent lymph flow through the superficial cervical lymph node.
- Define the cisterna chyli and describe its location and afferent and efferent lymph flow.
- Identify the thoracic duct on the left and right sides of the thoracic cavity and describe its lymph flow.
- Define a chylothorax.
- Describe the location of the tracheal trunks and the lymph flow through them.
- Define and identify the thymus.
Intercostal Arteries, Veins, and Nerves
-
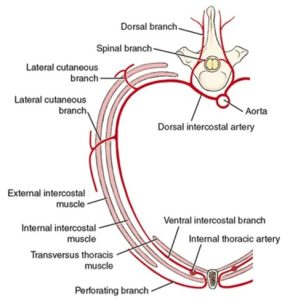
- Schematic transection of thoracic wall to show distribution of an intercostal artery. 1
-

- Intercostal arteries as seen within rib cage. 1
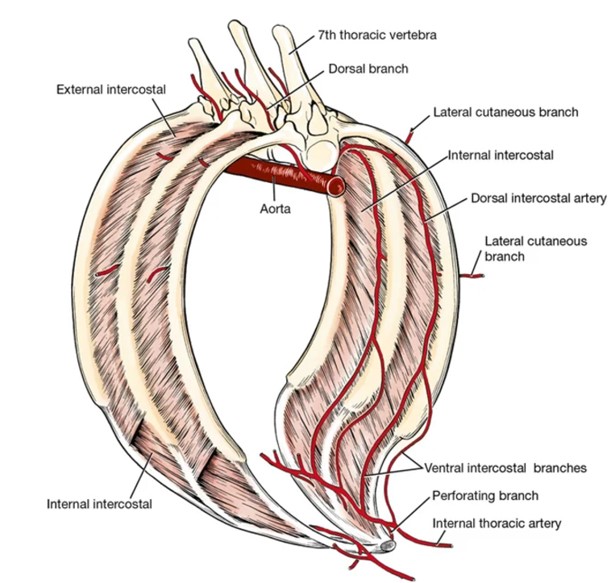
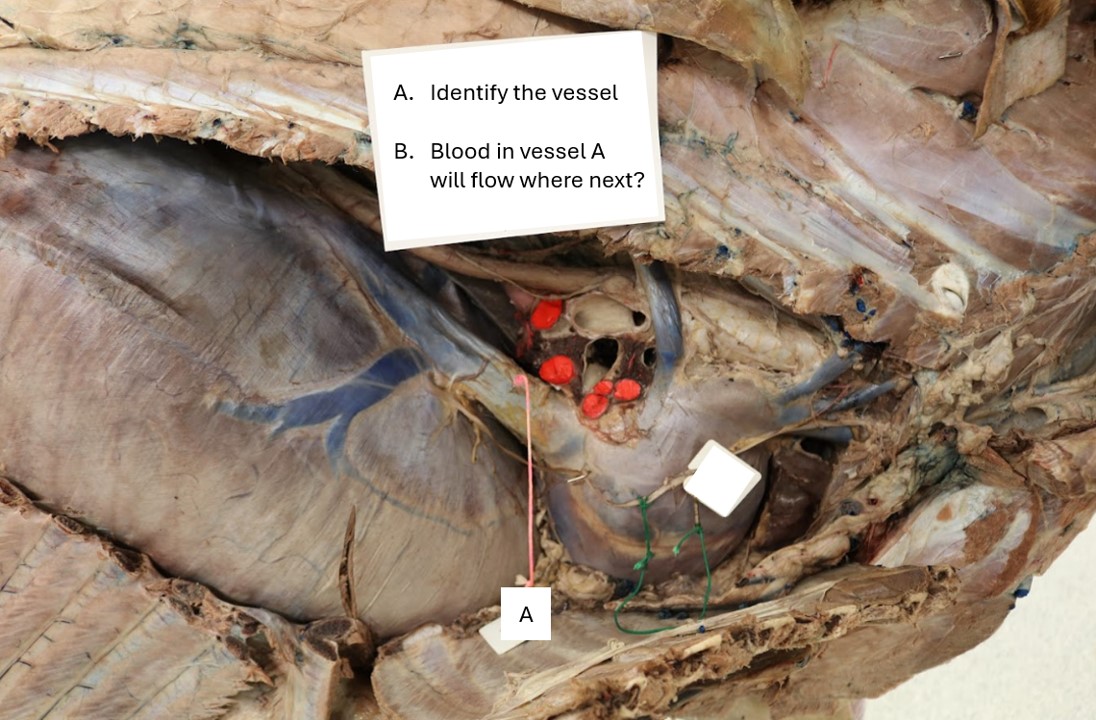
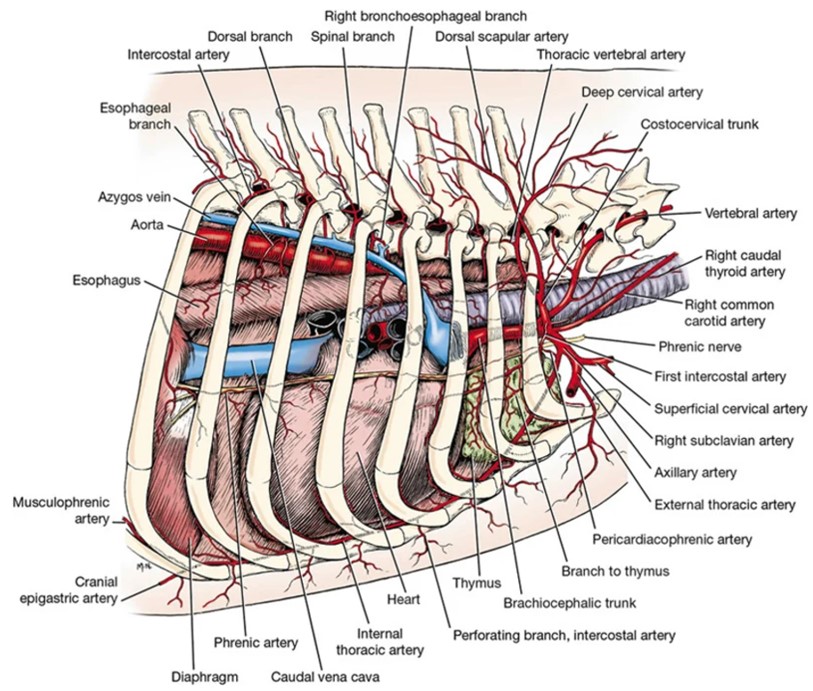
Observe: Before examining the thoracic wall nerves and vessels, study diagrams which show the pattern of distribution of these structures. Notice that the artery and nerve of each intercostal space divide into dorsal and ventral branches. The vessels and nerves are more readily identified on the deep surface of the thoracic wall – look for them there initially. On the external thoracic wall look for examples of cutaneous branches of intercostal nerves and vessels passing through muscles. As you read through the descriptions of these structures, identify them on the cadavers.
The first three dorsal intercostal arteries arise from a branch of the costocervical trunk while the remaining nine (in the dog) originate from the aorta. The ventral branches of the dorsal intercostal artery and vein pass ventrally, where they anastomose with ventral intercostal arteries, which have branched from the internal thoracic artery and vein (which we will dissect later). For our purposes, if asked to identify an intercostal artery, you will need not identify it as dorsal or ventral. However, you do need to know from where the dorsal and ventral intercostal arteries branch, i.e. most of the dorsal intercostal arteries branch from the descending aorta and the ventral intercostal arteries branch from the internal thoracic arteries.
FYI: At the ventral aspect of each intercostal space, another set of vessels called the perforating branches of the internal thoracic a. and v. emerge to supply cutaneous structures and the thoracic mammary glands (FYI). Dorsal and lateral rows of lateral cutaneous branches of intercostal nerves, and dorsal intercostal arteries, and veins emerge at regular intervals between the ribs and supply the cutaneous muscle, subcutaneous tissue, skin and thoracic mammae.
Clinical Application: Thoracocentesis
Thoracocentesis is a minimally invasive procedure whereby a needle is inserted into the pleural space to diagnose and/or treat pleural disease (fluid or air in the pleural cavity). Importantly, it is performed on the cranial aspect of the eighth or ninth rib, avoiding the neurovascular bundles (vein, artery, nerve) which are located on the caudal aspect of each rib. NCSU CVM Critical Care Clinical Skills Video
Veins cranial and dorsal to the heart
Dissect: Expose the larger veins cranial to the heart by carefully first cutting the first rib and reflecting it dorsally or removing it, if not done already. Then retract the sternum. Carefully incise and reflect the mediastinal parietal pleura to facilitate this exposure. The mediastinal parietal pleura is the thin, serous membrane covering the vessels in this location.
Clean and identify structures as you read through. Some structures have previously been identified and a few will be further described and identified in later sections.
The cranial vena cava drains into the right atrium after its formation by the union of the right and left brachiocephalic veins at the thoracic inlet. The brachiocephalic vein is formed on each side by the external jugular and subclavian veins. Usually the last branch entering the cranial vena cava is the azygos vein.
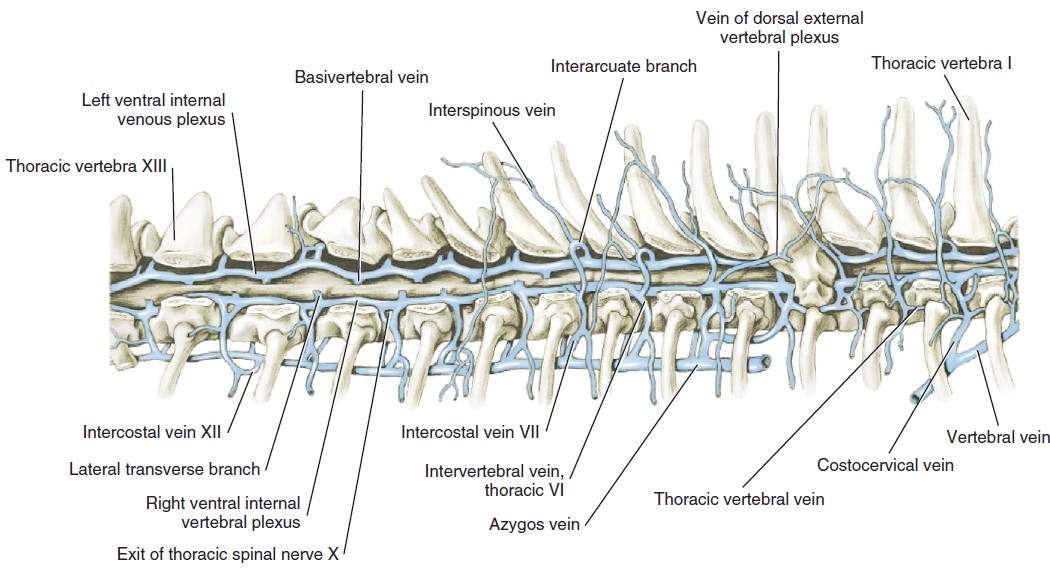
Only the right azygos vein develops in the dog and cat. The azygos vein may enter the right atrium directly. It is seen from the right in the mediastinal space winding cranioventrally around the root of the right lung. It originates dorsally in the abdomen and collects all of the dorsal intercostal veins on each side as far cranially as the third or fourth intercostal space.
Observe: Observe the azygous vein in the right thoracic cavity of the dog and cat.
-
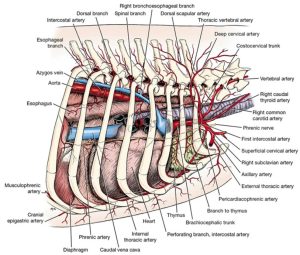
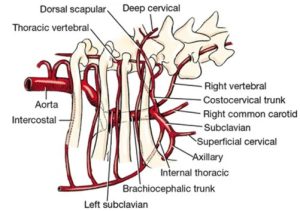
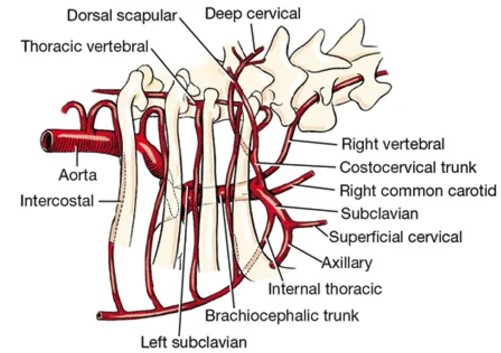
- Arteries of thorax of the dog, right lateral view. 1
-
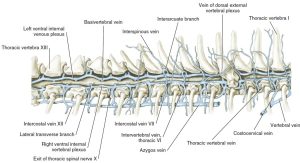
- Thoracic vertebral veins of the dog, right lateral aspect. 1

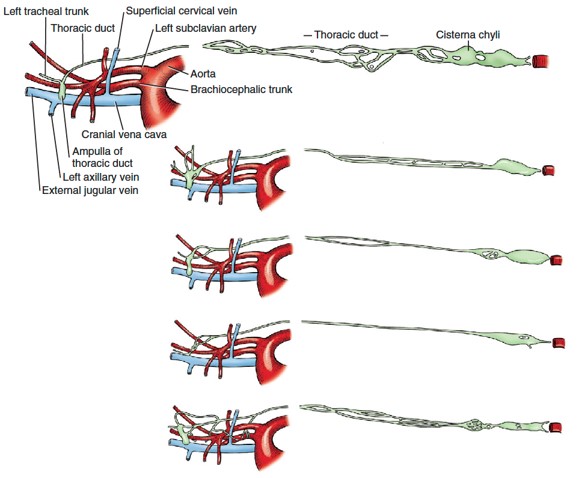
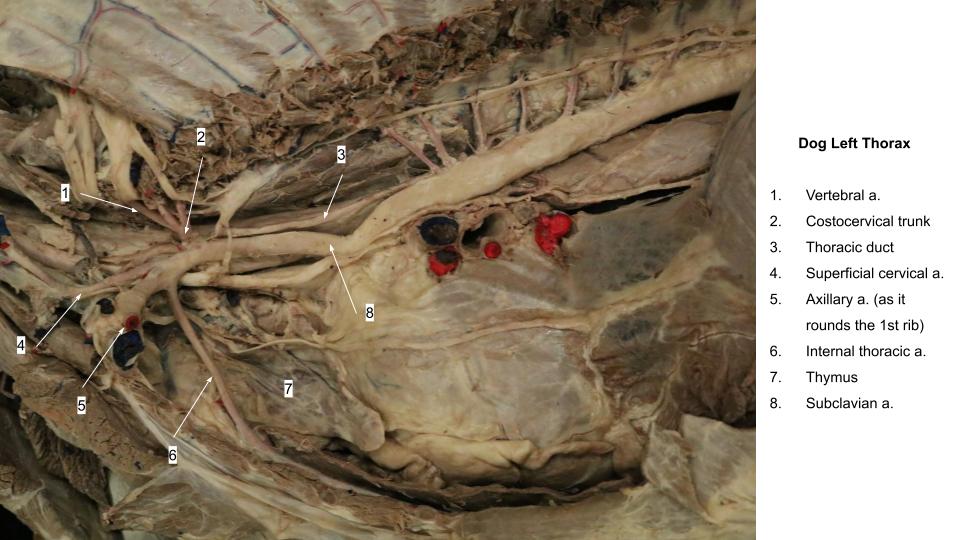
The thoracic duct is the chief channel for the return of lymph from lymphatic capillaries and ducts to the venous system. It begins in the sublumbar region between the crura of the diaphragm as a cranial continuation of the cisterna chyli. The latter is a dilated structure that receives the lymph drainage from abdominal and pelvic viscera and the pelvic limbs. The thoracic duct runs cranially on the right dorsal border of the thoracic descending aorta and the ventral border of the azygos vein to the level of the sixth thoracic vertebra (it may not be visible along this path). Here it crosses the ventral surface of the fifth thoracic vertebra and courses on the left side of the middle mediastinal pleura. It continues cranioventrally through the cranial mediastinum associated with the surface of the esophagus in this area, to reach the left brachiocephalic vein, where it usually terminates.
The thoracic duct also receives the lymph drainage from the left thoracic limb and the left tracheal trunk (from the left side of the head and neck). The lymph drainage from the right thoracic limb and the right tracheal trunk (from the right side of the head and neck) form a right lymphatic duct that enters the venous system in the vicinity of the right brachiocephalic vein. There are often multiple terminations of a complicated nature, which may include swellings or anastomoses. Lymphatic channels are difficult to see unless they are congested with lymph or refluxed blood. They are frequently double.
Dissect: Look for the thoracic duct on the left in the cranial thorax of your cadaver, crossing the esophagus. Locate it on the right side of the thorax in the caudal thorax. It is not always visible, but it may be identified by the reddish brown or straw color of its contents and the numerous random constrictions in its wall.
Review the location of the tracheal trunks, which may be found in each carotid sheath or parallel to the sheath and its contents. These lymphatic structures will be dissected and discussed again in the neck dissection.
-
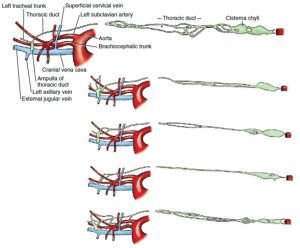
- variations of the thoracic duct of the dog and its entrance into the cranial vena cava. 1
-

- Dog thoracic duct
-
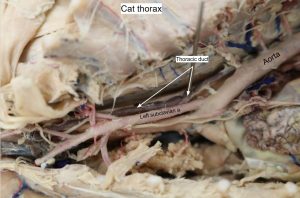
- Cat thoracic duct

Clinical Application: Chylothorax
- Chylothorax is a relatively rare condition in cats in which lymphatic fluid or chyle accumulates in the pleural cavity. The normally clear fluid in the pleural space has been replaced by chyle, a milky-white fluid from the thoracic duct. This unique fluid forms from lymphatic drainage of the intestinal tract, and is high in triglycerides, which gives it a distinct color and chemical composition. Normally, the thoracic duct transports chyle to the cranial vena cava for further processing by the body. With chylothorax, the chyle drains into the pleural space instead of the cranial vena cava. VCA Animal Hospitals.
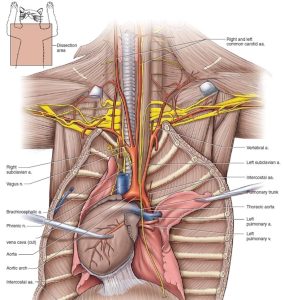
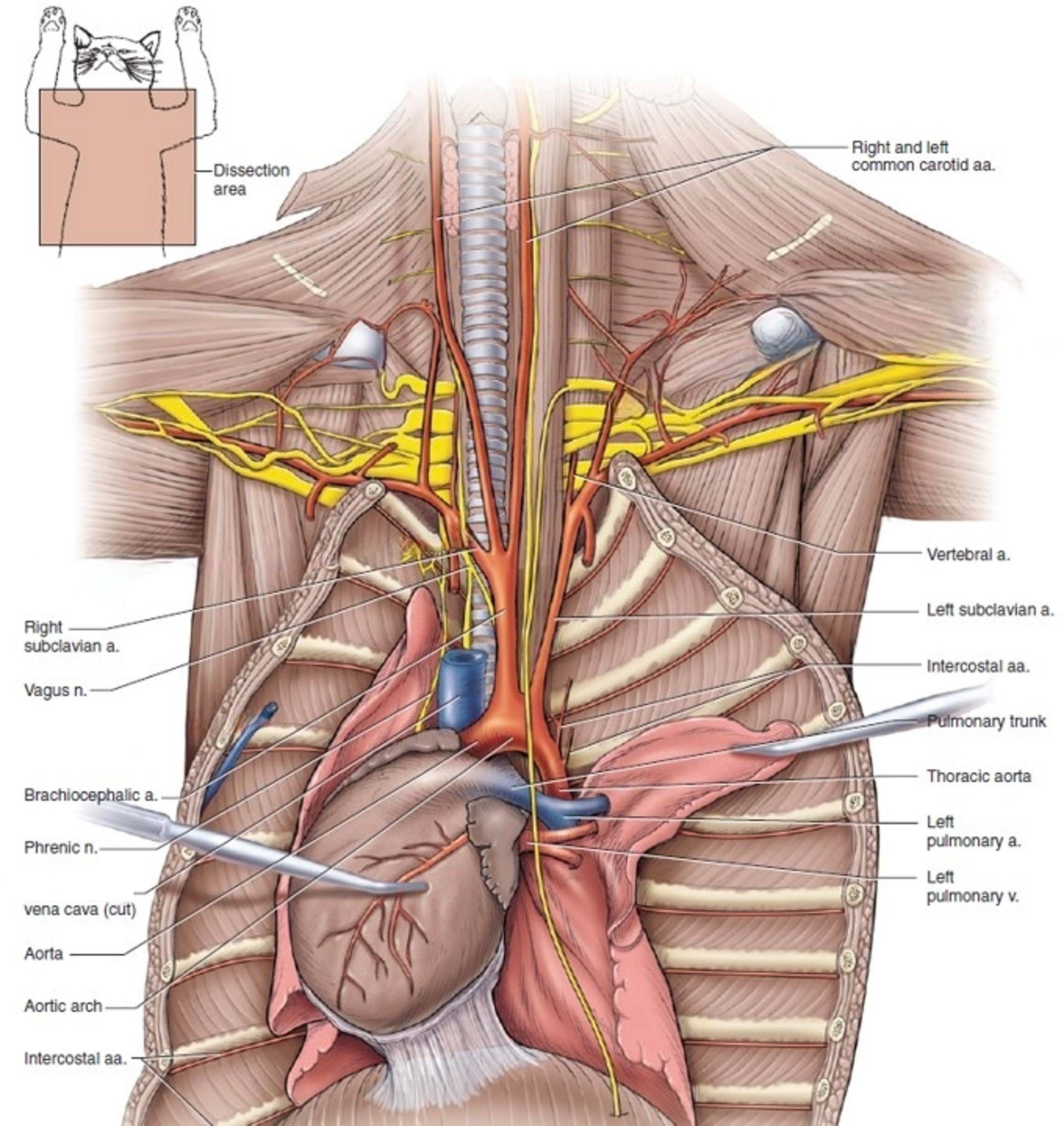
Arteries cranial to the heart
Dissect: Perform dissection of the following arteries on whichever side of your cadaver has been opened and observe the other side on prosections or on your groups’ cadavers, whichever is available. Clean and identify structures as you read through. Some structures have previously been identified and a few will be further described and identified in later sections.
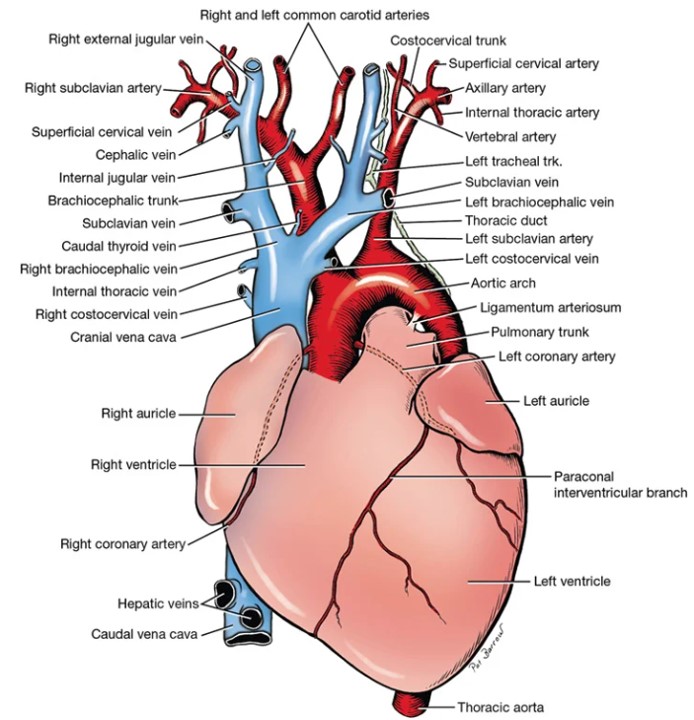
The aorta is the large, unpaired vessel that emerges from the left ventricle medial to the pulmonary trunk. The first short segment of the aorta is called the ascending aorta. It extends cranially from the aortic valve, covered by the pericardium. The aorta then makes a sharp bend dorsally and to the left as the slightly longer segment, the aortic arch. Distal to the aortic arch, the aorta runs caudally as the thoracic part of the descending aorta located ventral to the vertebrae. As the thoracic part of the descending aorta passes through the diaphragm into the abdominal cavity it becomes known as the abdominal descending aorta. Cranial to the heart are several branches of the aorta.
The right and left coronary arteries are branches of the ascending aorta that supply the heart muscle. They were studied with the heart.
The brachiocephalic trunk, the first branch from the aortic arch, passes obliquely to the right across the ventral surface of the trachea. It gives rise to the left common carotid artery and terminates as the right common carotid artery and the right subclavian artery.
The left subclavian artery is the second branch from the aortic arch exiting the vessel after the brachiocephalic trunk has done so. The branches of the right and left subclavian arteries are similar.
-
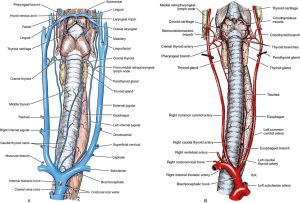
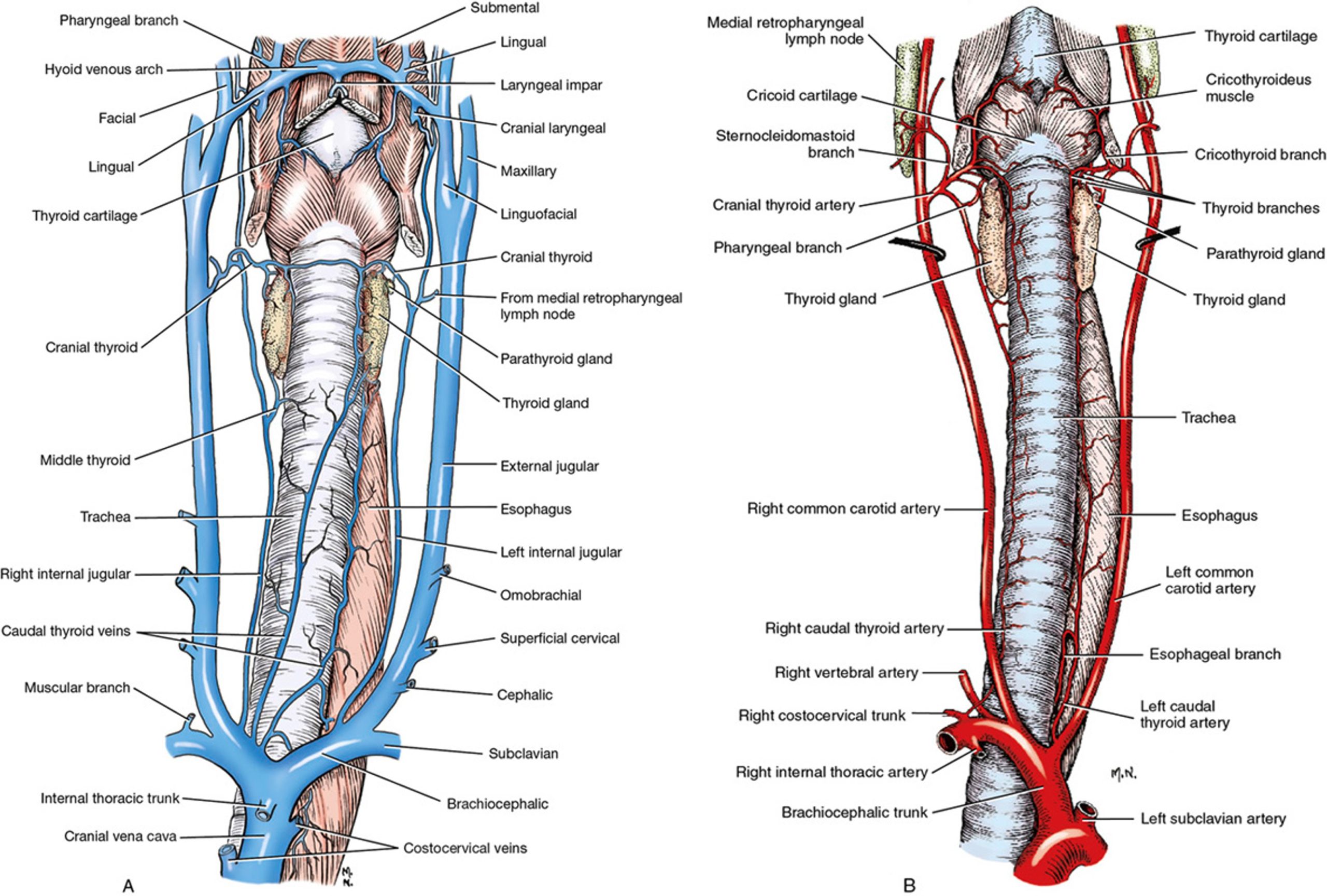
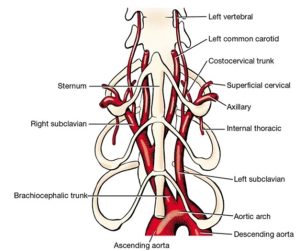
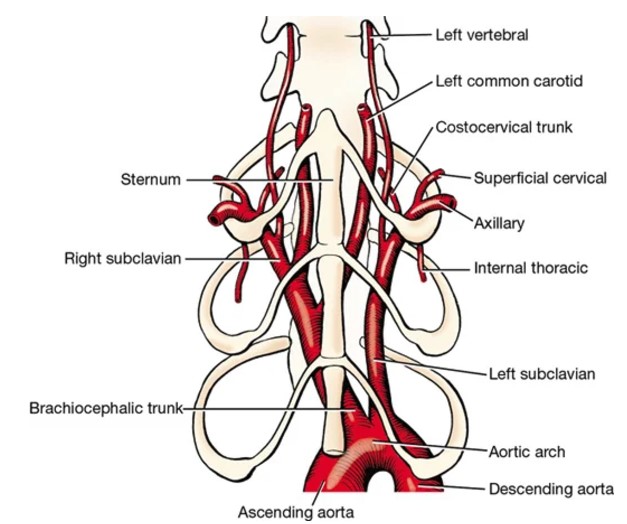
- Veins (A) and arteries (B) of the neck of the dog, ventral view. 1
-
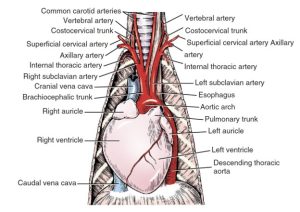
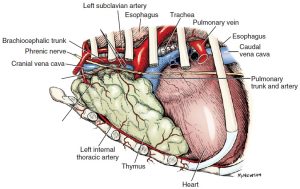
- Heart and great vessels of the dog, ventral view. 1
-
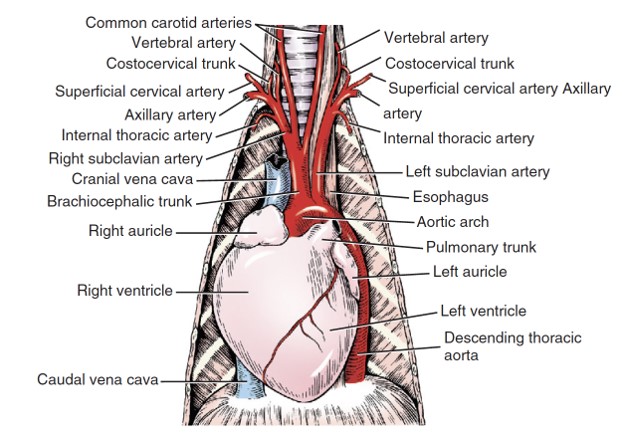
- Heart and great vessels of the dog (2), ventral view. 1
-
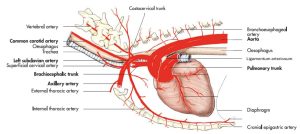
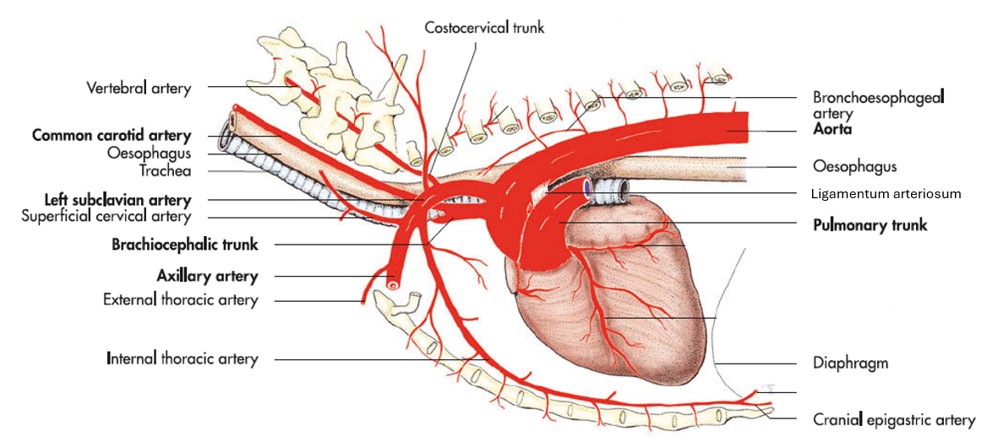
- Schematic illustration of the arteries cranial to the heart of the cat, ventral view. 5
-

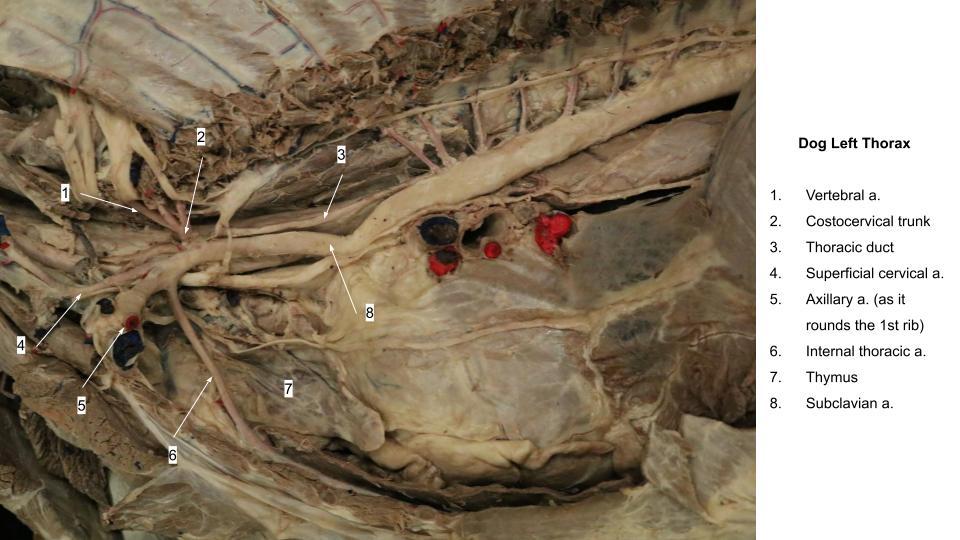
- Dog left lateral thorax

-
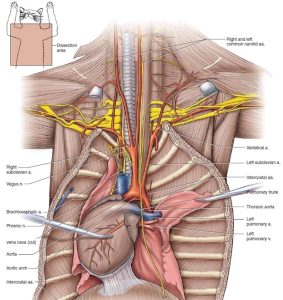
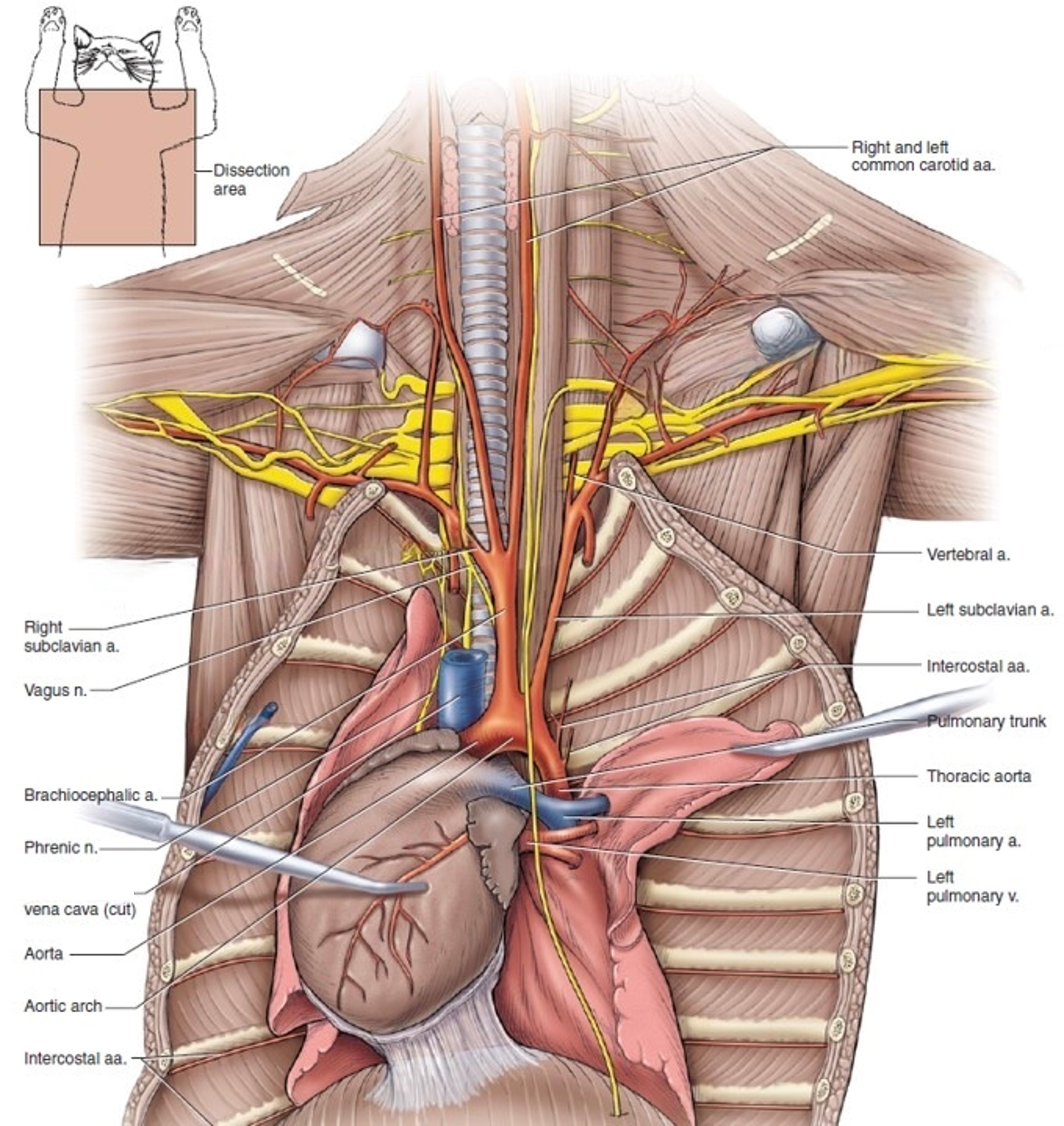
- Arterial, partial venous system and nerves anterior to the heart of the cat in ventral view.5
For each artery described, there is a comparable vein with a similar area of distribution. Be aware of but do not dissect the branches of the cranial vena cava. Again, the terminations of the veins are variable, and they will not be dissected. In fact, remove the veins when necessary to better visualize the arteries.
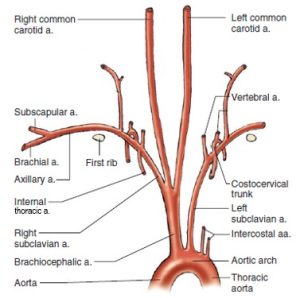
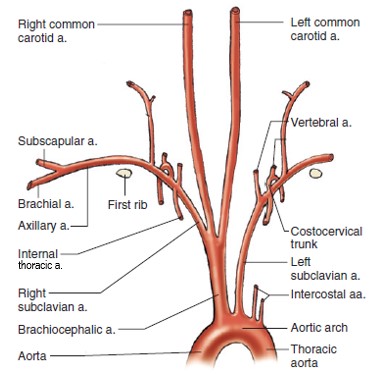
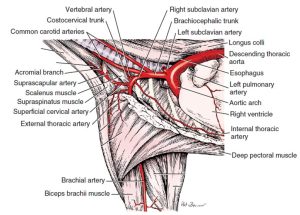
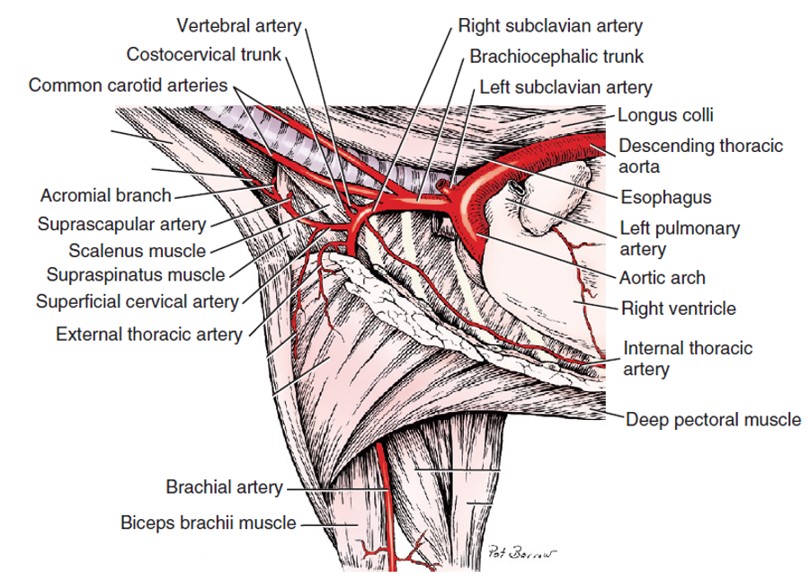
The left and right subclavian arteries each have four branches that arise medial to the first rib or intercostal space. They are the vertebral artery, the costocervical trunk, the superficial cervical artery, and the internal thoracic artery.
The vertebral artery crosses the medial surface of the first rib and disappears dorsally between the longus colli and the scalenus muscles. It enters the transverse foramen of the sixth cervical vertebra and passes through the transverse foramina of the first six cervical vertebrae. It supplies muscular branches to the cervical muscles and spinal branches at each intervertebral foramen to the spinal cord and its coverings. At the level of the atlas (C1), it terminates by entering the vertebral canal through the lateral vertebral foramen and contributes to the ventral spinal and basilar arteries.
The costocervical trunk arises distal to the vertebral artery, crosses its lateral side, and extends dorsally as far as the vertebral end of the first rib. By its various branches it supplies the structures of the first, second, and third intercostal spaces; the muscles at the base of the neck; and the muscles dorsal to the first few thoracic vertebrae.
The superficial cervical artery arises from the subclavian opposite the origin of the internal thoracic artery, medial to the first rib. It emerges from the thoracic inlet to supply the base of the neck and the adjacent scapular region. Observe the superficial cervical lymph node, to which the superficial cervical artery should lead.
The superficial cervical lymph nodes lie in the areolar tissue cranial to the shoulder. They lie deep to the cervical part of the cleidocephalicus and the omotransversarius and receive lymph drainage from the cutaneous area of the head, neck, and thoracic limb.
The internal thoracic artery leaves the subclavian artery, courses ventrocaudally in the cranial mediastinum, and disappears deep to the cranial border of the transversus thoracis m. It supplies many branches to surrounding structures—the phrenic nerve, the thymus, the mediastinal pleurae, and the intercostal spaces. Recall that the internal thoracic arteries give rise to the ventral intercostal arteries, which anastomose with the dorsal intercostal arteries. Near the attachment of the costal arch with the sternum, the internal thoracic a. terminates in the musculophrenic artery and the larger cranial epigastric a. The cranial epigastric artery and its cranial superficial epigastric branch will be observed in the abdomen section.
-
- Arteries of the cranial thorax and right thoracic limb of the dog, left lateral view. 1
-
- Veins (A) and arteries (B) of the neck of the dog, ventral view. 1
-
- Arteries of thorax of the dog, right lateral view. 1
-
- Branches of aortic arch of the dog, ventral view. 1
-
- Branches of brachiocephalic trunk of the dog, right lateral view. 1
-
- Arteries of the base of the heart and the cranial mediastinum of the dog. 6
-
- Arterial, partial venous system and nerves anterior to the heart of the cat in ventral view. 5
-
- Schematic illustration of the arteries cranial to the heart of the cat, ventral view. 5
-
- Dog thoracic duct
Branches of the thoracic descending aorta
The esophageal and bronchial arteries vary in number and origin. Usually the small bronchoesophageal artery leaves the right fifth intercostal artery close to its origin and crosses the left face of the esophagus, which it supplies. There may be a left and a right bronchoesophageal artery (or only one). The artery(ies) may also branch directly from the descending aorta. Regardless, the bronchoesophageal arteries(y) terminates shortly afterward in the bronchial arteries, which supply the lung.
Also recall there are eight to nine pairs of dorsal intercostal arteries that leave the descending aorta. These start with either the fourth or the fifth intercostal artery and continue caudally, there being an artery in each of the remaining intercostal spaces. Each lies close to the caudal border of the rib. The costocervical trunk supplies the first three or four intercostal spaces.
Clean and identify the bronchoesophageal artery (only on the left side) and dorsal intercostal arteries (you need only see one or two) as they branch from the thoracic descending aorta.
-
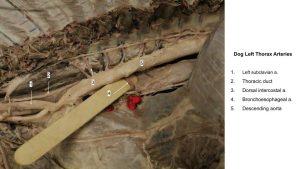
- Dog broncoesophageal artery

Thymus
The thymus is a bilobed, compressed structure situated in the cranial mediastinum. It is largest in the young dog and usually atrophies with age until only a trace remains. When maximally developed, the caudal part of the thymus is molded on the cranial surface of the pericardium. The thymus is the organ primarily responsible for the production and maturation of T cells of the immune system.
Observe: Observe the thymus, if it is still present in your cadaver.
-
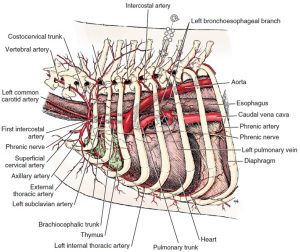
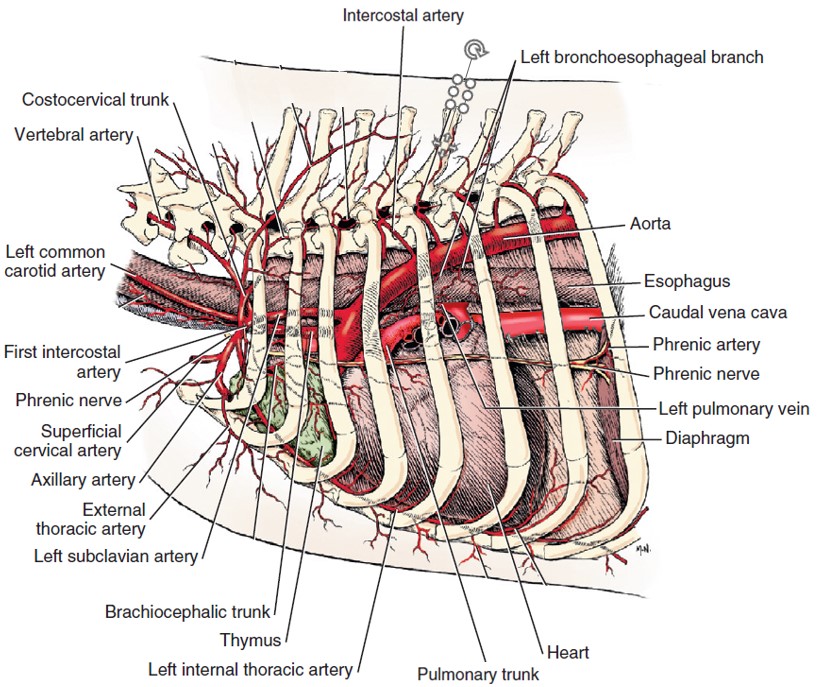
- Arteries of thorax of the dog, left lateral view. 1
-
- Arteries of thorax of the dog, right lateral view. 1
-
- Thymus of a young dog. 1
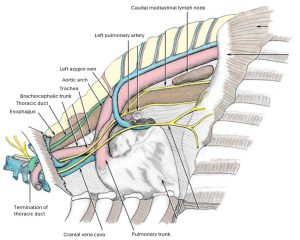
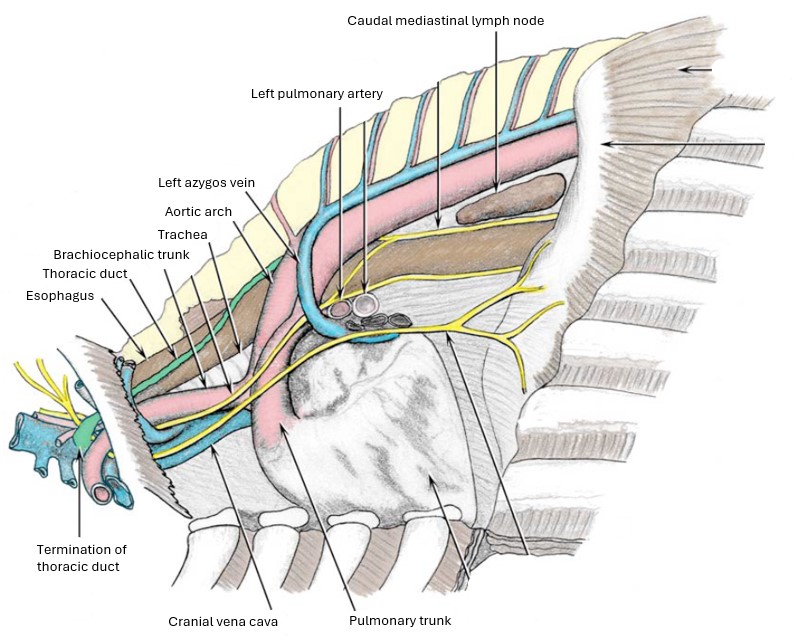
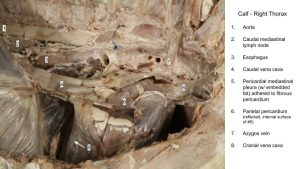
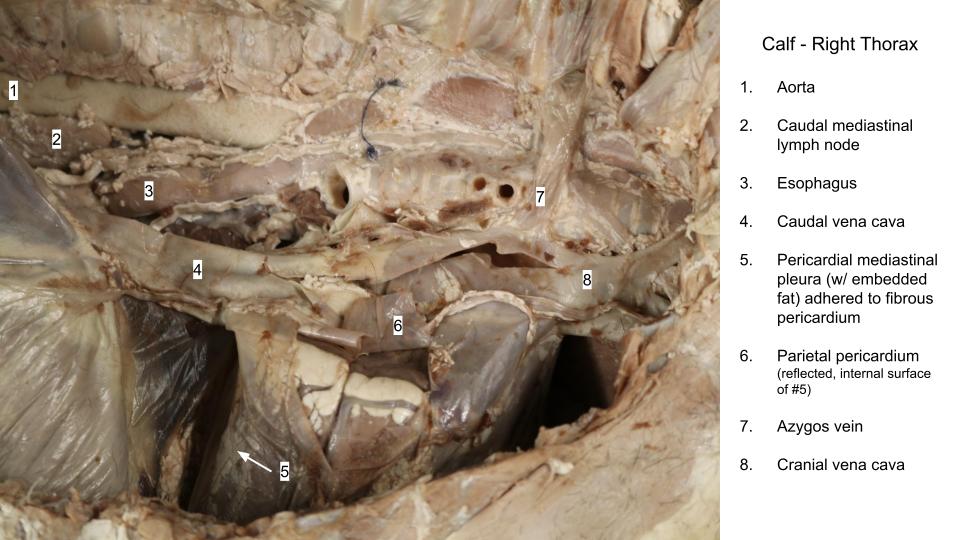
Vasculature of the Thoracic Cavity Ungulate Highlights
Observe: Examine the internal surface of the thoracic wall to identify the intercostal neurovascular structures passing on the caudal margin of each rib. Identify the intercostal a., v., n.
Observe: Observe the following structures in the ungulate species, as described below.
Identify the thoracic duct (don’t bother in the calf) passing over the left side of the esophagus heading toward its termination in the convergence of large veins near the thoracic inlet. The thoracic duct may be partially filled by blue latex that has retrofluxed into the duct from the venous system. You need not identify the thoracic duct on the right side, but take care not to confuse it for other structures, especially in the horse, where it can be quite large.
Identify the thymus in the cranial mediastinum. The thymus of the horse involutes early in life, whereas in the ruminant, it remains relatively more obvious in the adult.
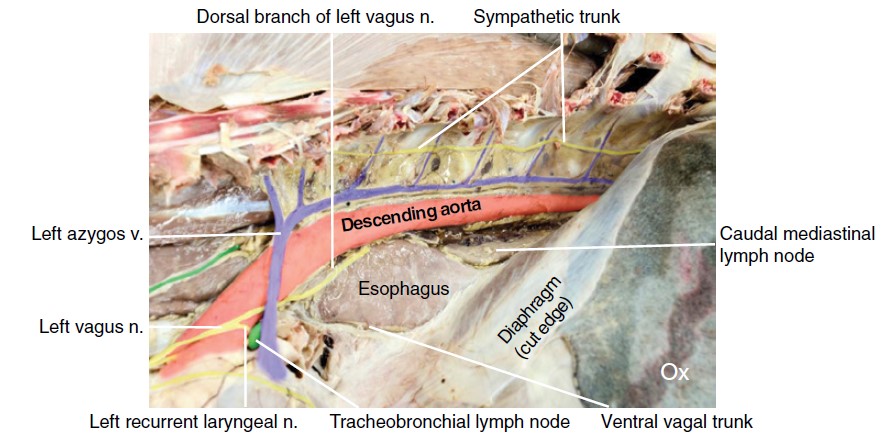
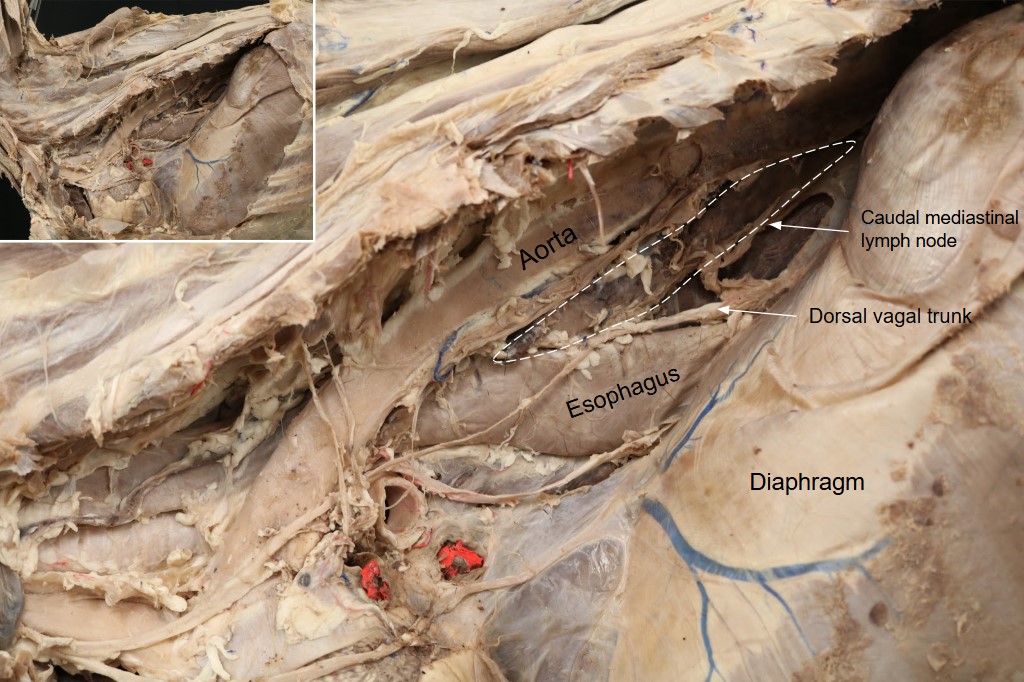
In the ruminants, caudal mediastinal lymph nodes are of particular clinical importance; identify these nodes located between the esophagus and aorta in the caudodorsal mediastinum.
The tracheobronchial lnns. are found immediately dorsal to the lung hilus.
Identify the azygos vein(s), cranial and caudal vena cava, and descending aorta in the ungulate species. The caudal vena cava can be observed on the right side of the thorax. The azygous vein is consistently present on the right side of the equine. Note that in the artiodactyls, the left azygos vein is consistently present and passes cranial to the hilus of the left lung and then curves caudally to enter the right atrium at the coronary sinus. Occasionally, a complete right azygos vein is also present in the ox, but in most cases this vein represents only the cranial part of
an azygos vein. While it is not necessary to memorize on which side the azygos (sometimes spelled azygous) is present (it won’t be asked on a written exam, for example), it may help with identification to remember where to expect it.
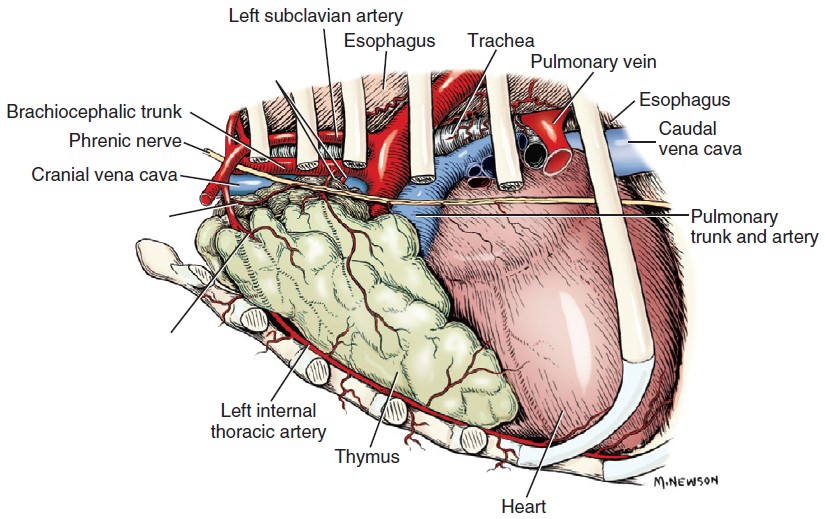
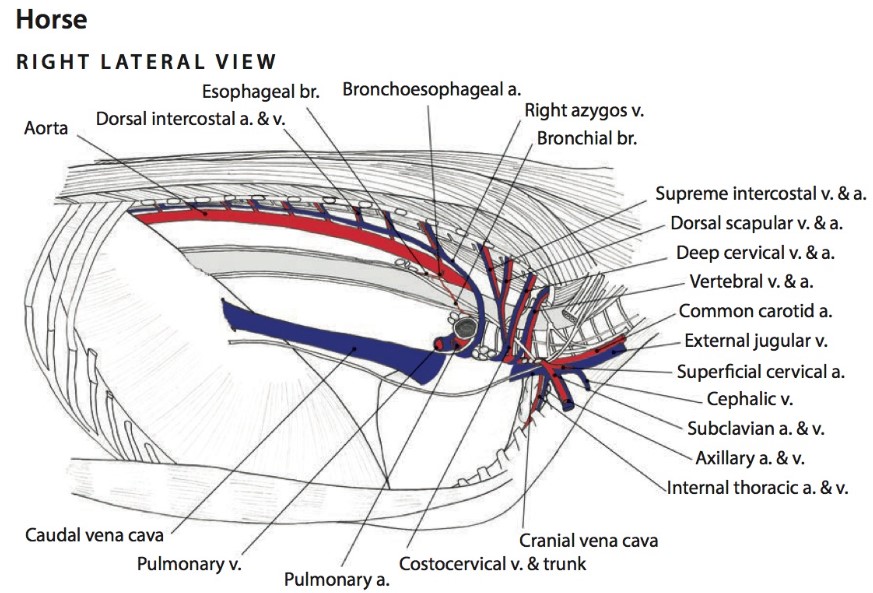
Horse
-
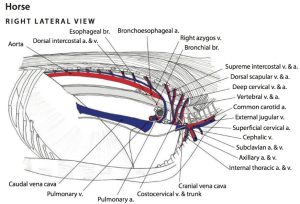
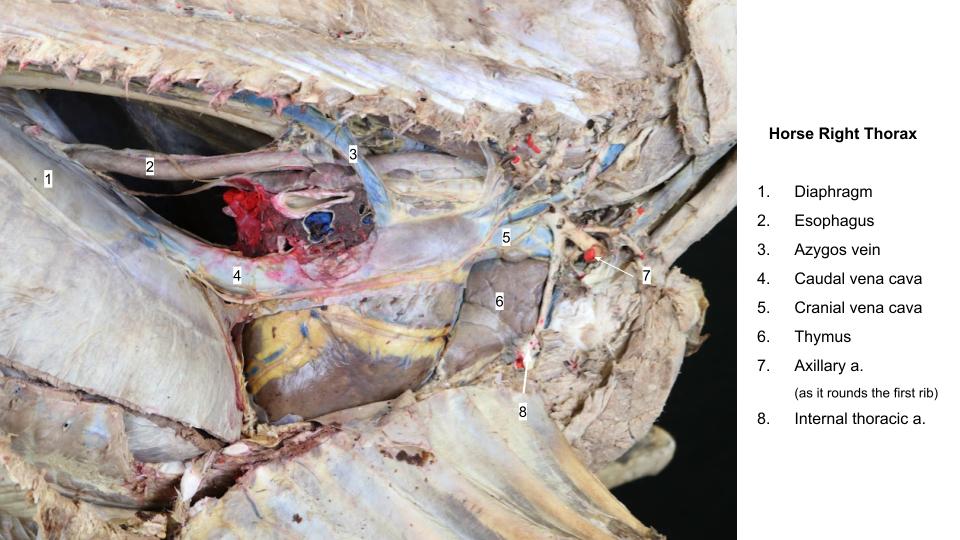
- Vessels of the thoracic cavity of the horse, right side.6
-
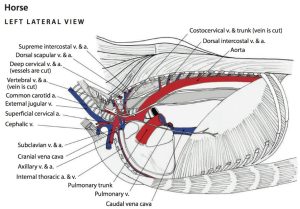
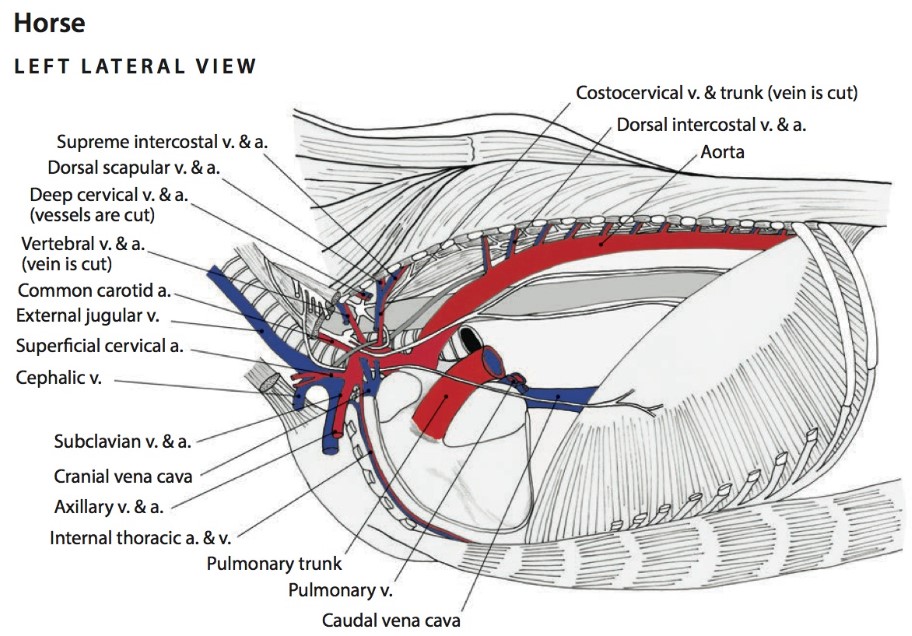
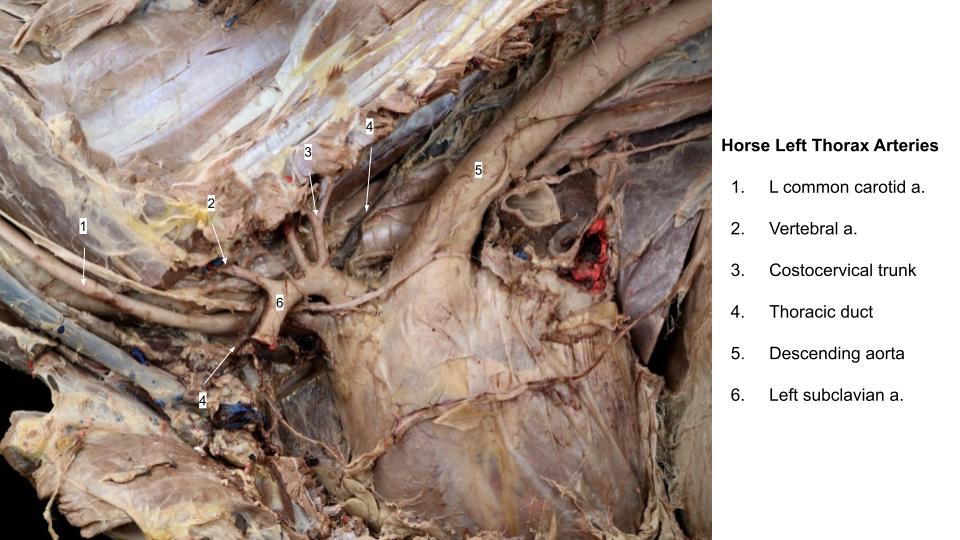
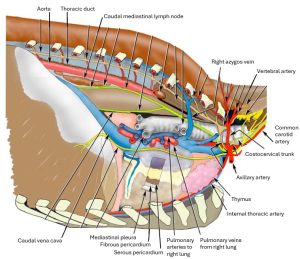
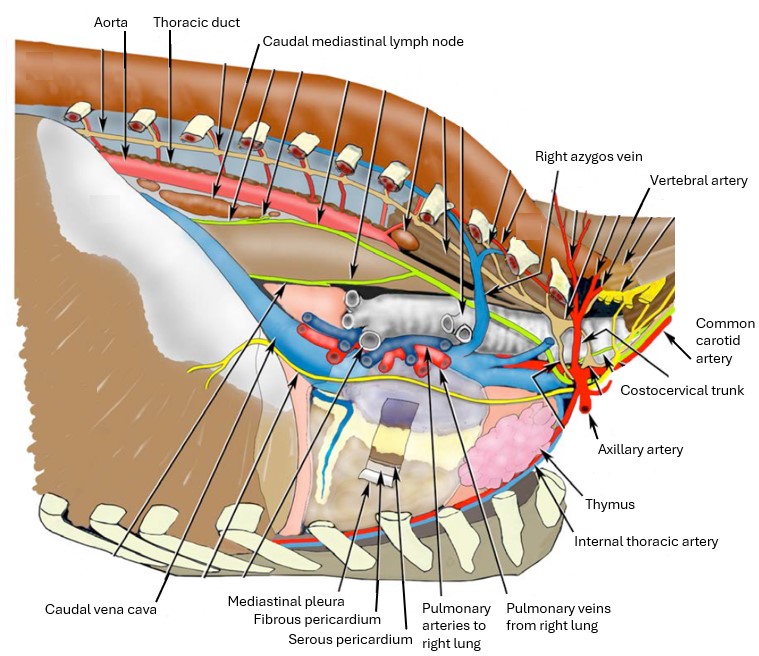
- Vessels of the thoracic cavity of the horse, left side.6
-
- Blood vessels at the base of the heart of the horse. 6
-
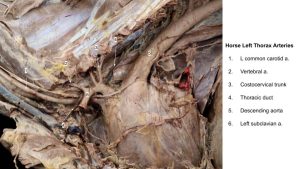
- Horse left thorax
-

- Horse right thorax
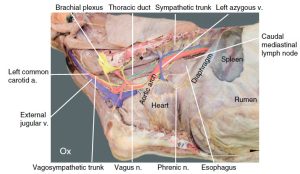
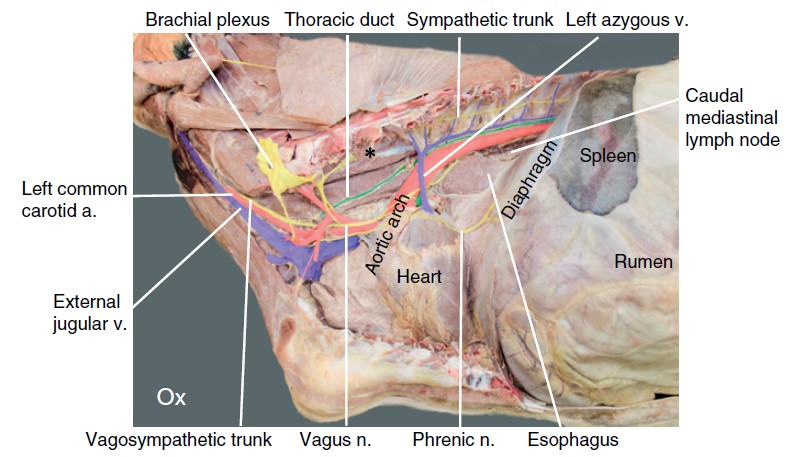
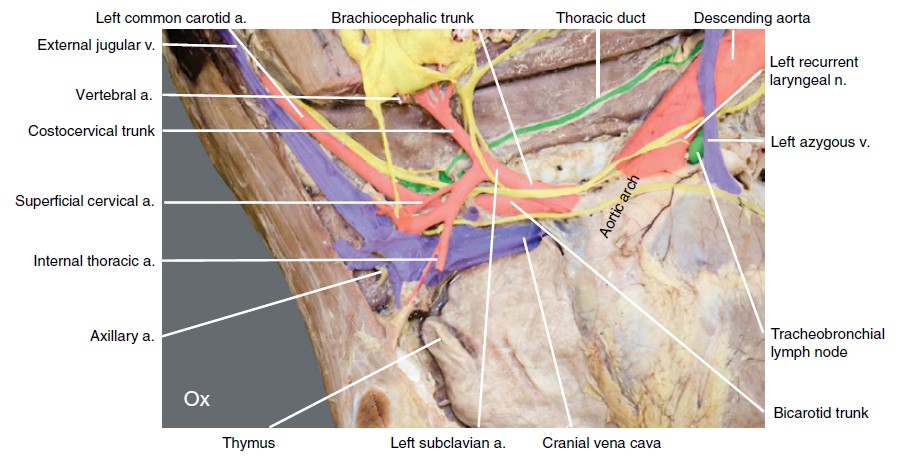
Ox
-
- Major arteries of bovine mediastinum, right lateral view. 2
-
- Major structures of bovine mediastinum, left lateral view. 2
-
-
Bovine left thoracic and cranial abdominal cavities. Identify the major vessels and nerves on the
left thoracic cavity. 12
-
- Bovine left thorax (cranial part). 12
-
- Bovine left caudal thorax. 12
-
- Calf thorax vessels
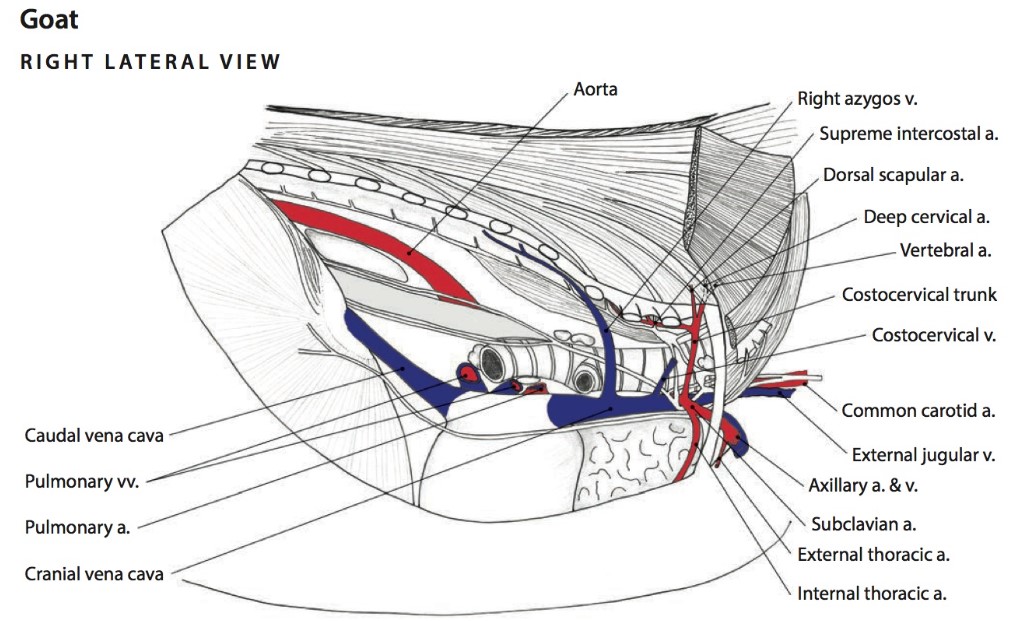
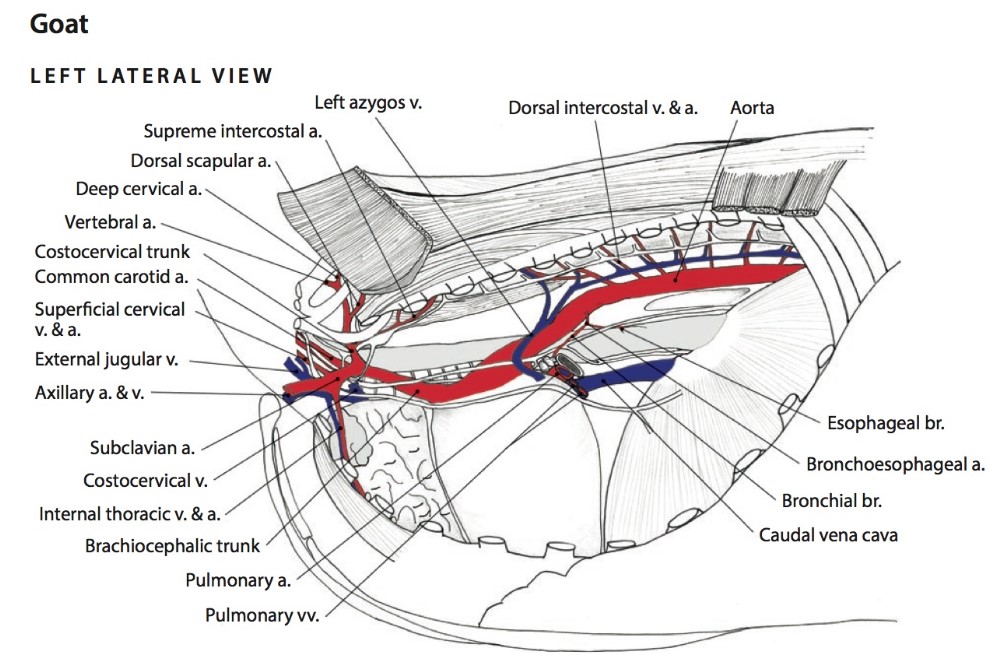
Goat
-

- Vessels of the thoracic cavity of the goat, right side. 6
-
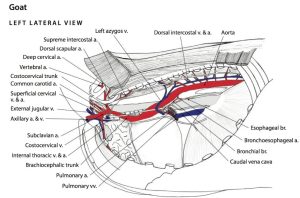
- Vessels of the thoracic cavity of the goat, left side.6
Clinical Application: Caudal mediastinal lymph node enlargement (lymphadenopathy)
The caudal mediastinal lnn., when enlarged, can compress the esophagus and result in bloat. Such enlargement can also damage the vagal trunks and interfere with normal gastric motility.
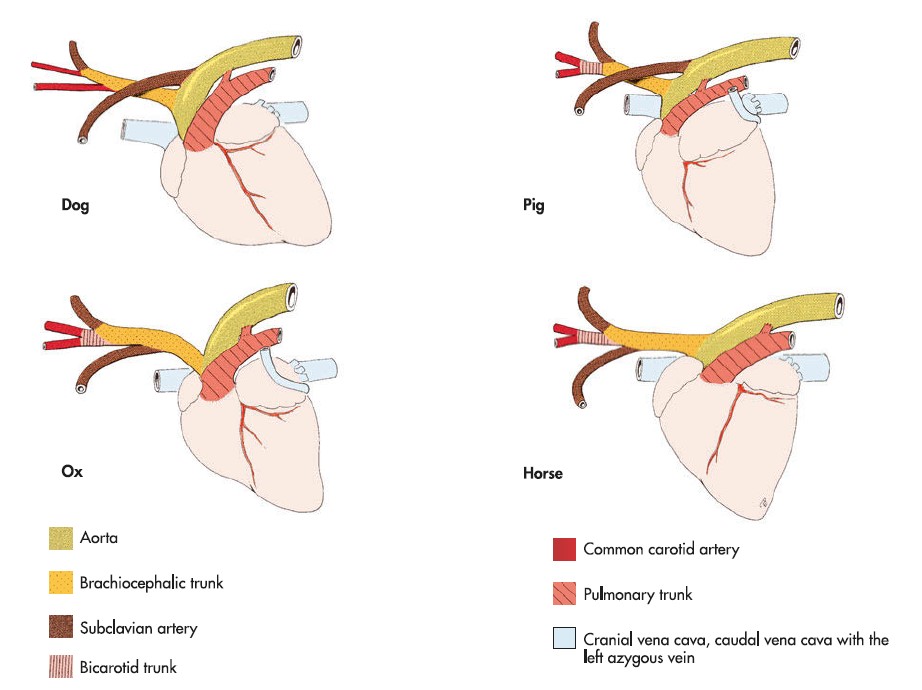
Observe: You are not responsible for identifying the great vessels of the heart in situ in the large animal species. However, you should be aware that they branch differently from the aorta in the equine and ruminant than they do in the carnivore and pig. As you recall from your study of the carnivores, the two major branches of the aortic arch (after the coronary arteries) are the brachiocephalic trunk and left subclavian artery – and pigs follow a similar plan.
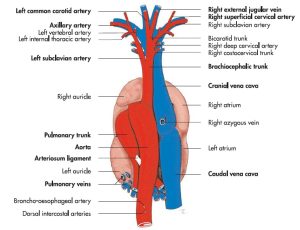
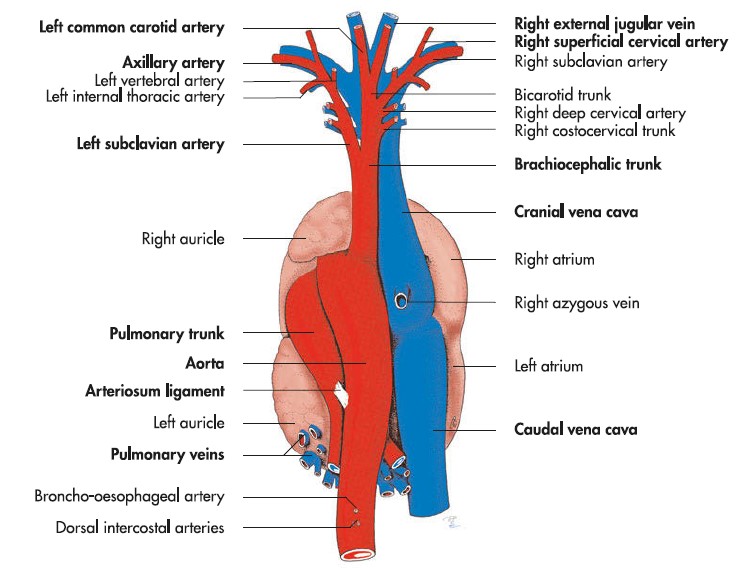
For the horse and ruminant, the only branch of the aortic arch is the brachiocephalic trunk. The left and right subclavian arteries typically arises as branches of the brachiocephalic trunk, as does the bicarotid trunk, which then gives rise to the right and left common carotid arteries. See the diagram below for a comparative study of the arteries. Where present on ex situ specimens, identify the brachiocephalic and bicarotid trunks and the left and right subclavian arteries.
-
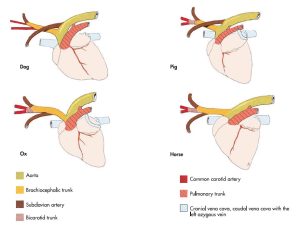
- Comparison of the vessels at the base of the heart of the domestic mammals. 7
Review videos
Dog thoracic arteries, 6 min – Watch until 13:50
Goat thoracic vessels left, 1 min – Watch until 9:00
Goat thoracic vessels right, 2 min – Watch until 14:30
Calf thoracic vessels, right – 6 min
Terms
| Heart and Thorax |
|
| Features | Species |
| Aorta | All |
| Ascending aorta | All |
| R coronary a | All, (observe in heart dissection) |
| L coronary a | All, (observe in heart dissection) |
| Aortic arch | All |
| Descending aorta | All |
| Brachiocephalic trunk | All |
| Bicarotid trunk | Equine and ruminant ex situ, if possible. Know conceptually regardless. |
| Intercostal aa/vv | All. Know where dorsal and ventral IC arteries originate. |
| Bronchoesophageal a/v | Carnivore only |
| L/R Subclavian a/v | Carnivore only |
| Vertebral a/v | Carnivore only |
| Costocervical trunk | Carnivore only |
| Superficial cervical a/v | Carnivore only |
| Internal thoracic a/v | Carnivore only |
| Ventral intercostal aa/vv | Know from where they originate. |
| Cranial epigastric a/v | Do not ID. Know it is continuation of internal thoracic a |
| Common carotid aa | All |
| Cranial vena cava | All |
| Caudal vena cava | All |
| Azygos v | Right – carnivore, horse, ruminant (when present in ruminant) Left – pig, ruminant |
| Cisterna chyli | Do not ID. Define, know location, and direction of lymph flow through it. |
| Thoracic duct | All left side. Right side on dog/cat if possible. Know where it is located, and efferent and afferent flow. |
| Chylothorax | Define and name most common domestic species. |
| Tracheal trunks | Do not ID until next lab. Know where they are and what they drain. |
| Superficial cervical lymph node | All. Know afferent and efferent flow. |
| Thymus | All (where present) |
| Caudal mediastinal lymph node | Ruminants. Know what secondary clinical signs may arise from caudal mediastinal lymphadenopathy. |
| Tracheobronchial lymph nodes | Ungulates |