Lab 2A: Upper Respiratory Tract 2 – Larynx and Trachea
Learning Objectives
- Describe the function of the larynx and recognize its relationship with the laryngopharynx and nasopharynx
- Describe and identify the structures of the larynx – cartilages, muscles, folds, and other features, and recognize species differences
- Describe the anatomy of glottis abduction – muscle, cartilages, joint, nerve
- Identify the cervical trachea and tracheal cartilages
- Associate the normal anatomy with clinical conditions and procedures
Lab Instructions
The limited dissection required is performed by teams on carnivore cadavers. Otherwise much of the content is also learned on available lab prosections and models, wet and dry. The bolded terms are to be specifically identified. Additional context and terminology is provided to provide a complete overview of the anatomy. Once the carnivore material has been considered, move to the ungulate specimens to learn comparative features and to complete the learning goals.
Larynx – overview
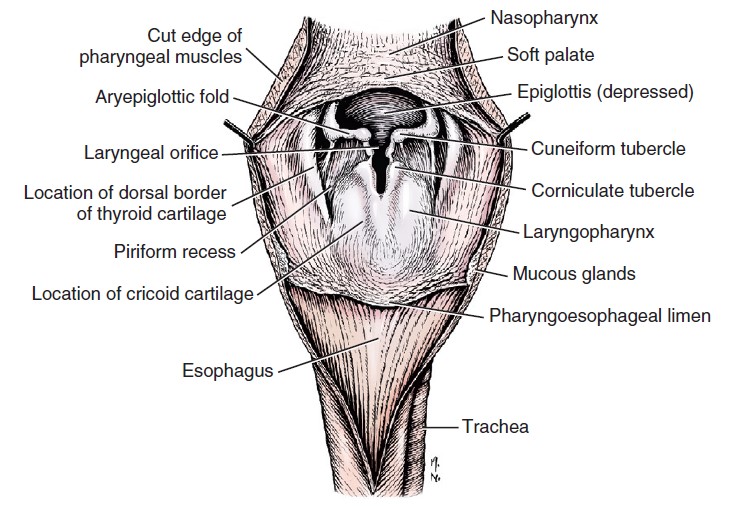
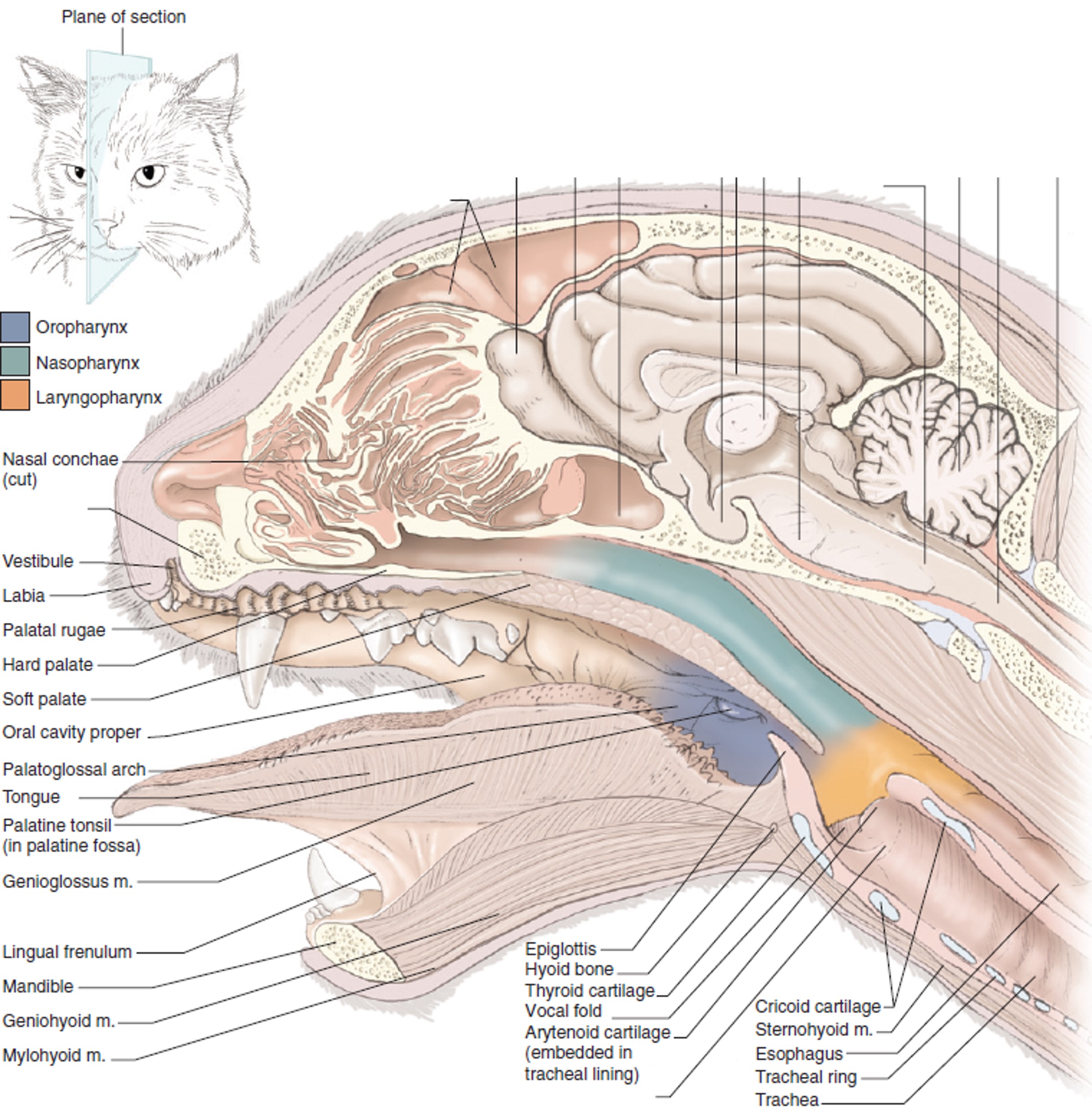
The larynx is that part of the upper respiratory tract situated between the nasopharynx and the trachea. It is the site of voice production, the pathway for air to enter the trachea, and it seals off the lower airway during swallowing. The larynx consists of integrated cartilages, muscles, ligaments, and is lined internally by respiratory mucosa. Innervation and blood supply are extensive. The larynx projects rostrally into the space of the laryngopharynx, which recall from Lab 1A, is the part of the pharynx that continues the oropharynx and nasopharynx. The laryngopharynx functions mostly to channel swallowed fluids and food towards the esophagus. When the animal is not swallowing, respired air passes through the rostral space of the laryngopharynx (this depends on the species and refer to the horse below), entering and leaving the larynx. On either side of the entrance to the larynx, the laryngopharynx forms a channel known as the piriform recess (there is a left and right piriform recess). The piriform recesses represent the rostral part of the laryngopharynx, and run lateral to the epiglottis and arytenoid cartilages and their intervening aryepiglottic fold. The recesses are continued dorsal to the larynx by the common space of the laryngopharynx, which subsequently ends at its junction with the esophagus. During swallowing, the recesses provide a channel for ingested food and liquids to pass by the closed off larynx.
-
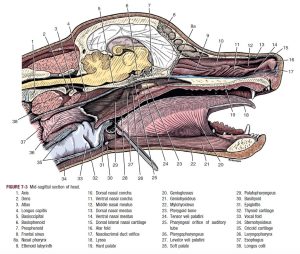
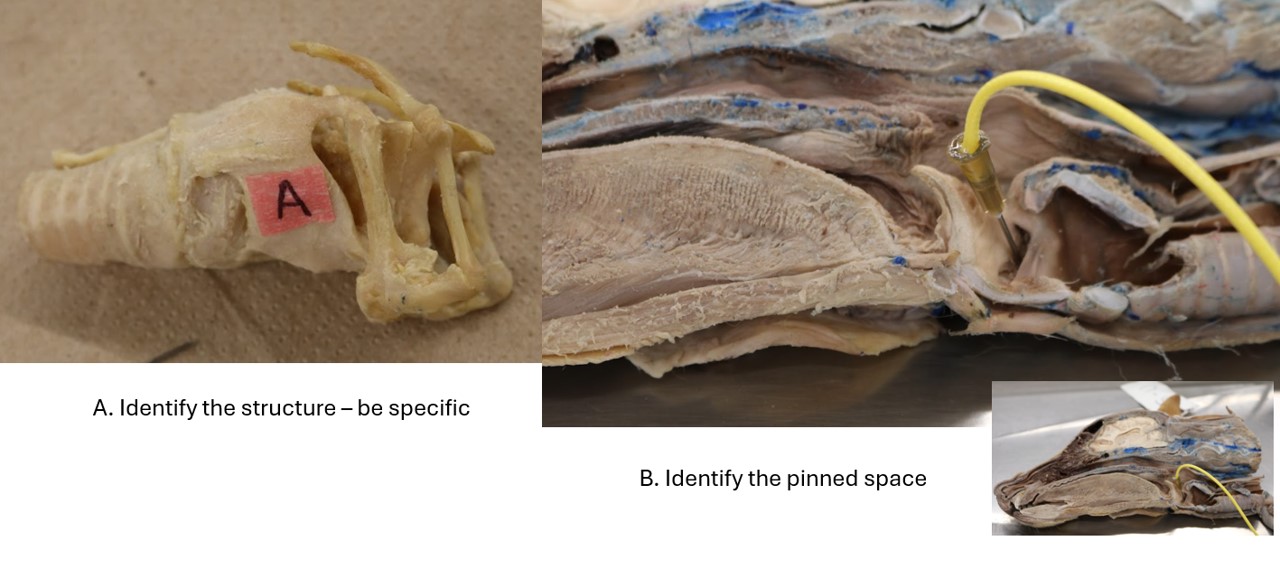
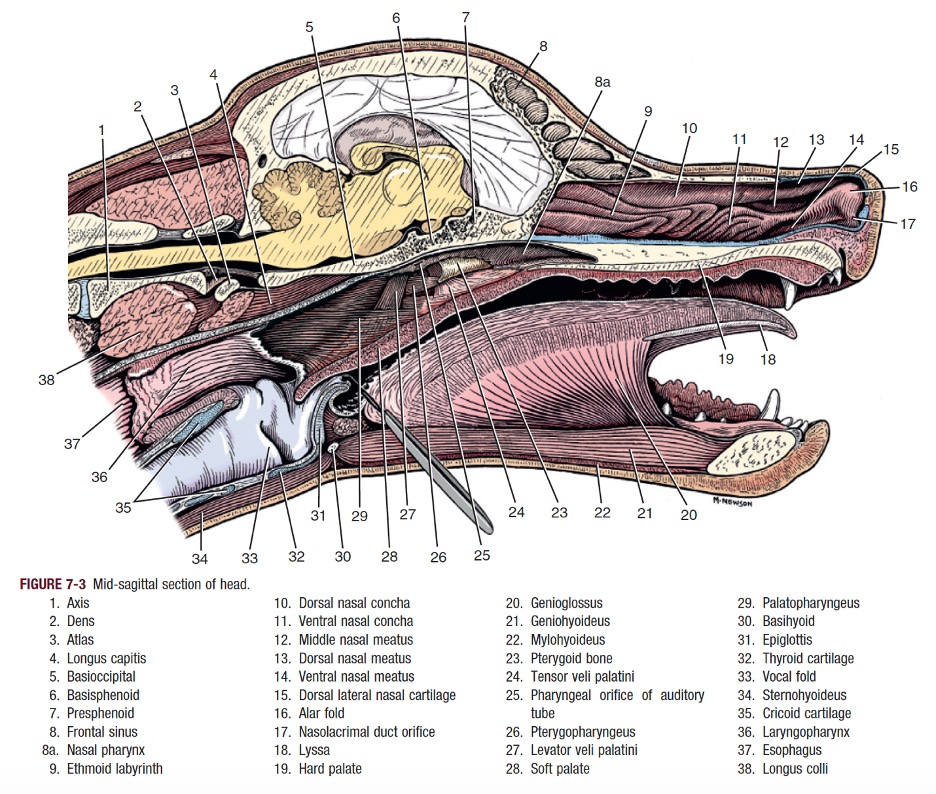
- Canine midline section of head.1
-
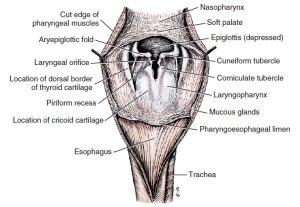
- The pharynx of the dog opened middorsally. 1
-
- Sagittal section of the cat head. 5
Clinical Application – piriform recesses
Structures attempting to be swallowed (rigid food, like a bone, or foreign bodies) may lodge in the piriform recesses.
Cartilages of the larynx (Cartilagines laryngis)
There are four cartilages of the larynx. Located rostral to caudal they are the epiglottis, the paired arytenoid cartilage, the thyroid cartilage, and the cricoid cartilage. The unpaired cartilages will be considered first.
The epiglottis is the leaf- or spade-shaped cartilage that lies at the entrance to the larynx. Its lingual (deep) surface is attached to the basihyoid bone and faces the oropharynx. The apex of the epiglottis usually sits just dorsal to the caudal edge of the soft palate. On each side, the lateral margin is attached by a mucosal fold to the arytenoid cartilage to form the aryepiglottic fold. In the cat this fold extends further to attach to the cricoid cartilage. Caudally, the epiglottis attaches at its base, to the body of the thyroid cartilage.
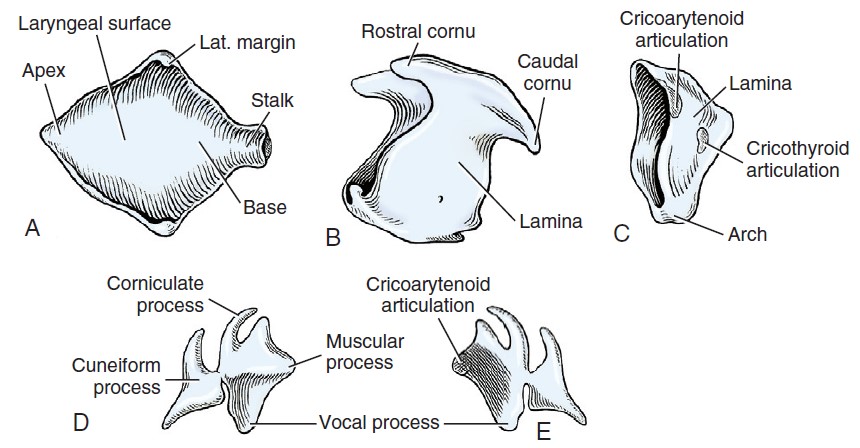
The thyroid cartilage, shaped like a boat’s hull, forms a deep trough, which is open dorsally. The laminae of the thyroid cartilage (the lateral sides of the ‘boat hull’) lie to the outside of the arytenoid cartilages. The rostral cornu (horn) articulates with the thyrohyoid bone; the caudal cornu articulates with the caudal aspect of the cricoid cartilage. Ventrally, the caudal border is characterized by a median caudal thyroid notch.
The caudally-located cricoid cartilage forms a complete ring that lies partially within the trough of the thyroid cartilage. It has a wide dorsal plate, or lamina, and a narrow ventral arch. Near the caudal border at the junction of the lamina and the arch, there is a lateral facet for articulation with the caudal cornu of the thyroid cartilage (forming the cricothyroid joint). On the cranial border of the lamina, there is a prominent pair of lateral facets for articulation with the arytenoid cartilages, forming the cricoarytenoid joint. On ventral midline, the space between the ventral arch of the cricoid cartilage and the caudal, notched border of the thyroid cartilage is bridged by the cricothyroid ligament.
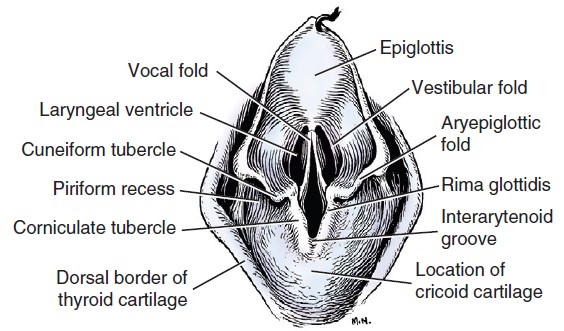
The arytenoid cartilage is paired, irregular in shape, and located in the sagittal plane. Each cartilage has a medial facet that articulates with the lateral facet on the rostral border of the cricoid lamina, forming the critical, aforementioned cricoarytenoid joint. Dorsally the left and right arytenoid cartilages are connected by a short transverse ligament. There are up to four processes associated with each arytenoid cartilage, with species variation. The dog has all four and these are the cuneiform process, corniculate process, muscular process, and vocal process. The cuneiform process is the most rostral projection and supports the aryepiglottic fold and the vestibular fold in the dog. Just caudal to the cuneiform process, the corniculate process projects dorsally. Laterally, the muscular process provides an attachment site for the dorsal cricoarytenoideus m., the critical abductor of the glottis – see below. Lastly, the ventrally directed vocal process provides attachment for the vocal ligament and vocal muscle. The vocal ligament and muscle are covered by mucosa, which forms the vocal fold. The vocal fold passes from the vocal process of the arytenoid to the midventral part of the thyroid cartilage. The vestibular fold lies immediately rostral to the vocal fold, and extends from the thyroid cartilage ventrally, to the ventral portion of the cuneiform process dorsally. Between the vestibular and vocal folds is a narrow opening, in the dog, that is the entrance to the laryngeal ventricle. The laryngeal ventricle is a diverticulum (outpouching) of the laryngeal mucosa bounded laterally by the thyroid cartilage and medially by the arytenoid cartilage. It may have a role in modulating voice sounds.
Note that in the cat, the cuneiform and corniculate processes of the arytenoid cartilages are not present. There are no distinct vestibular folds in the cat’s larynx and no laryngeal ventricle. However, they most certainly still have vocal folds, ligaments and muscles!
Observe: the vocal and vestibular folds and the laryngeal ventricle on the medial side of laryngeal specimens of the dog. In the cat, identify the vocal fold.
-
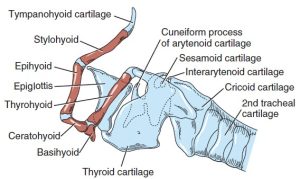
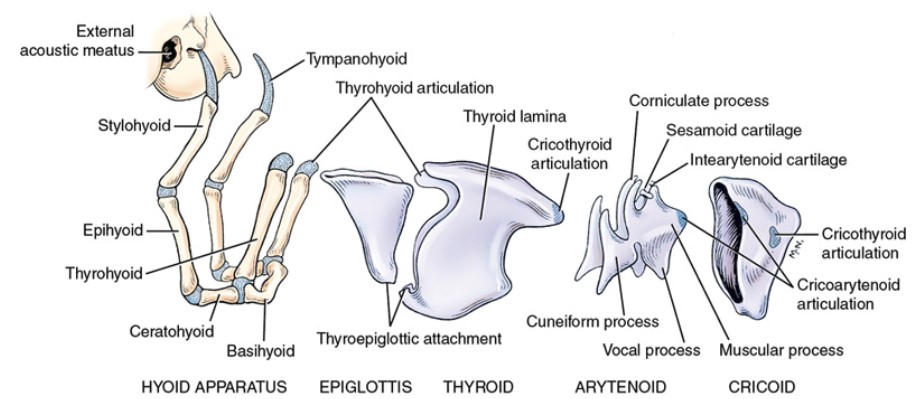
- Hyoid apparatus, larynx, and trachea of the dog, left lateral view. 1
-
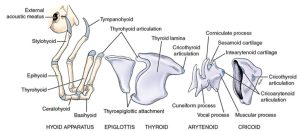
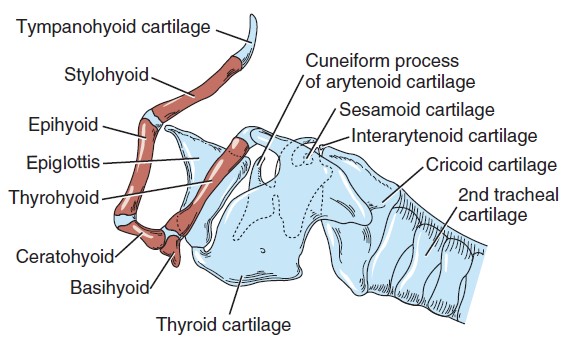
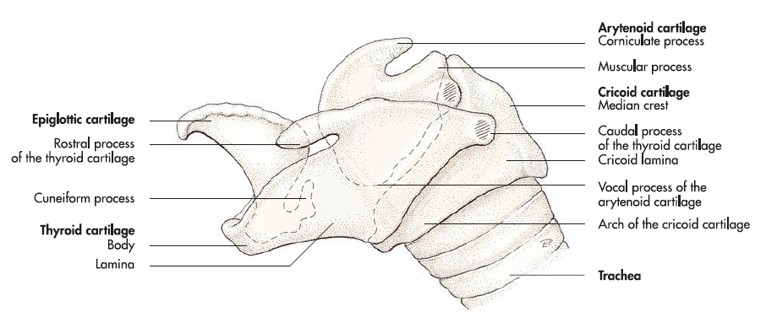
- Cartilages of the disarticulated larynx of the dog with hyoid apparatus intact, left lateral view. 1
-
-
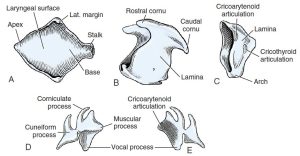
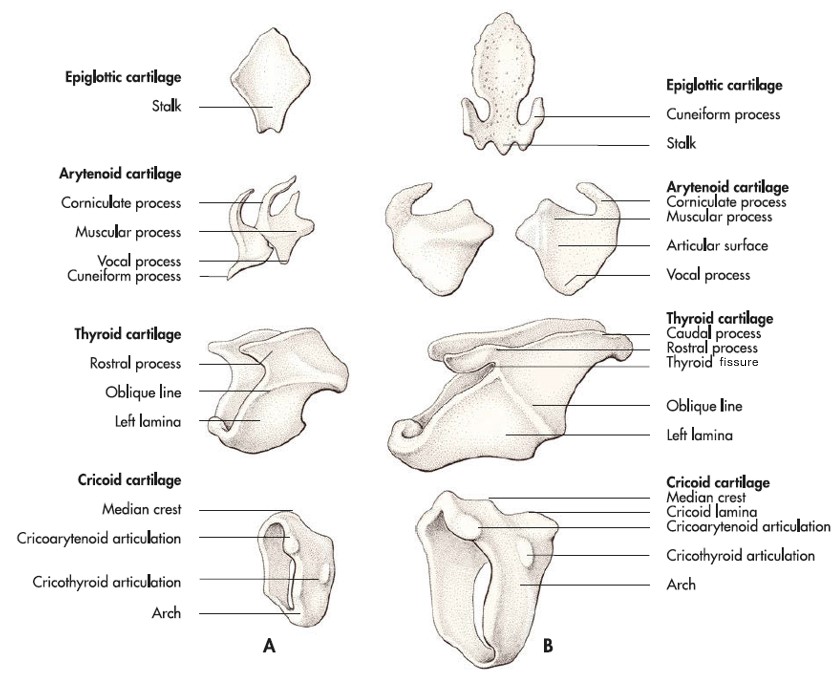
Laryngeal cartilages of the dog, disarticulated. A, Epiglottis, dorsal aspect. B, Thyroid cartilage, lateral aspect.
C, Cricoid cartilage, lateral aspect. D, Left arytenoid cartilage, lateral aspect. E, Left arytenoid cartilage, medial aspect. 1
-
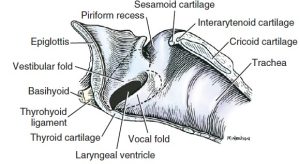
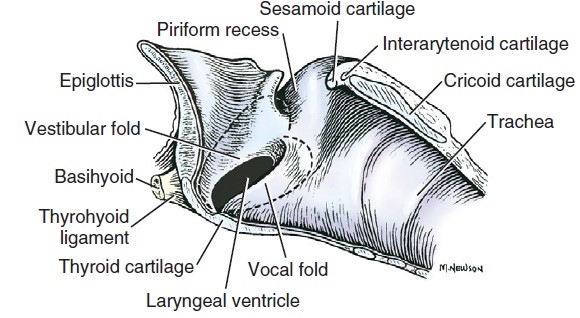
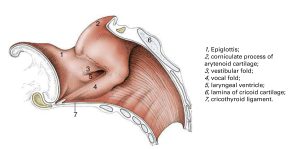
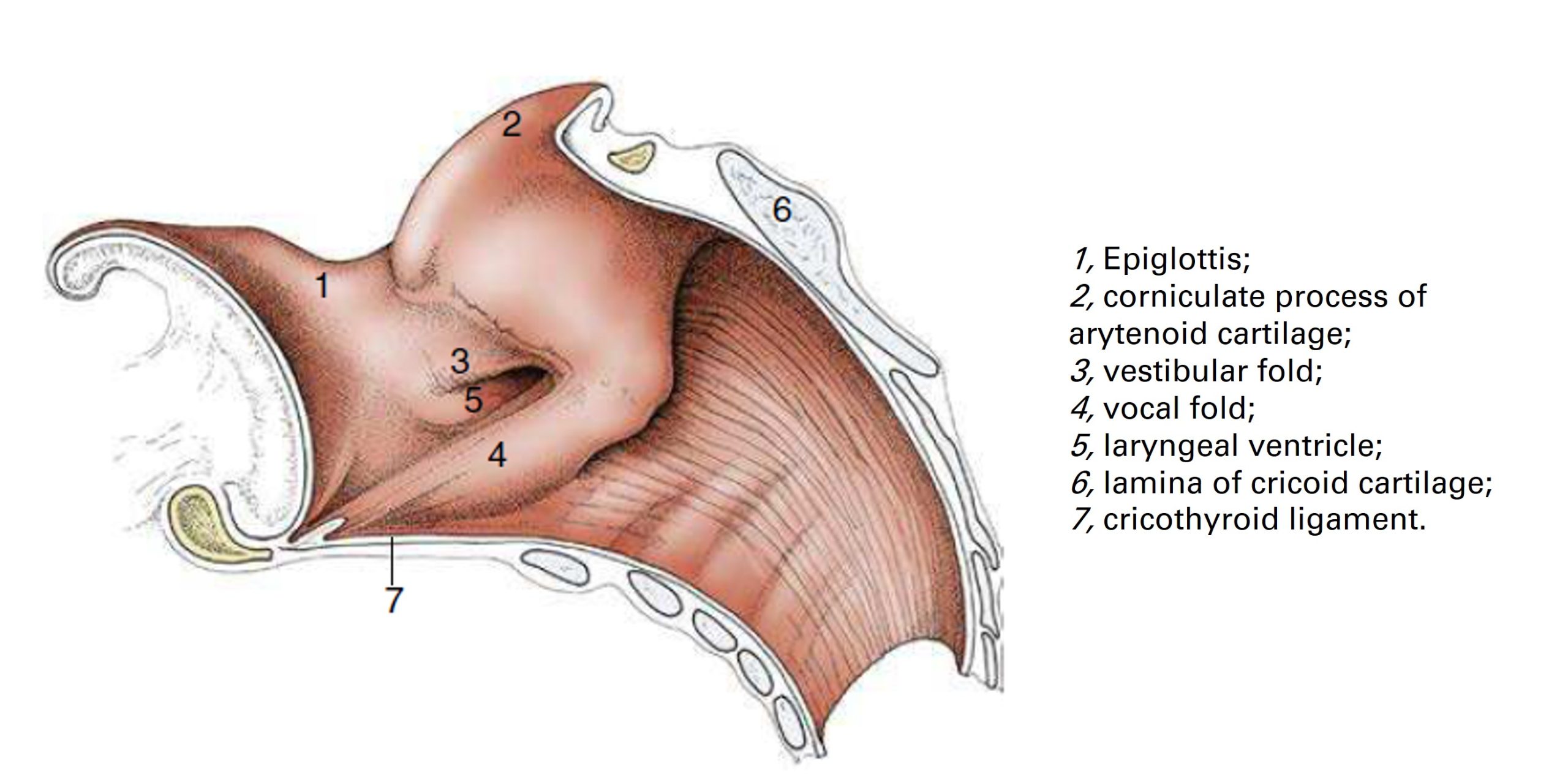
- Median section of the larynx of the dog. (The dotted lines show the extent of the laryngeal ventricle.) 1
-
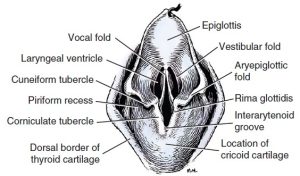
- Dorsal aspect of larynx of the dog, showing vocal and vestibular folds. 1
-
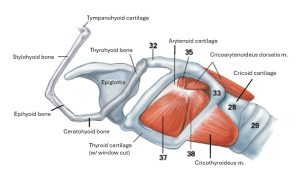
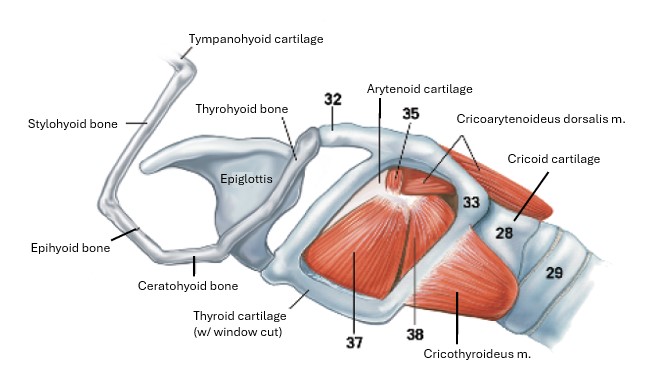
- Intrinsic musculature of larynx of the cat, lateral view with window in thyroid cartilage. 4
Clinical application – vocal folds and ventriculocordectomy
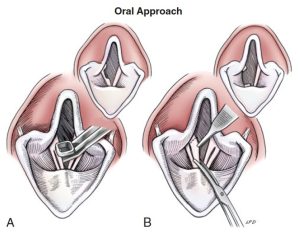
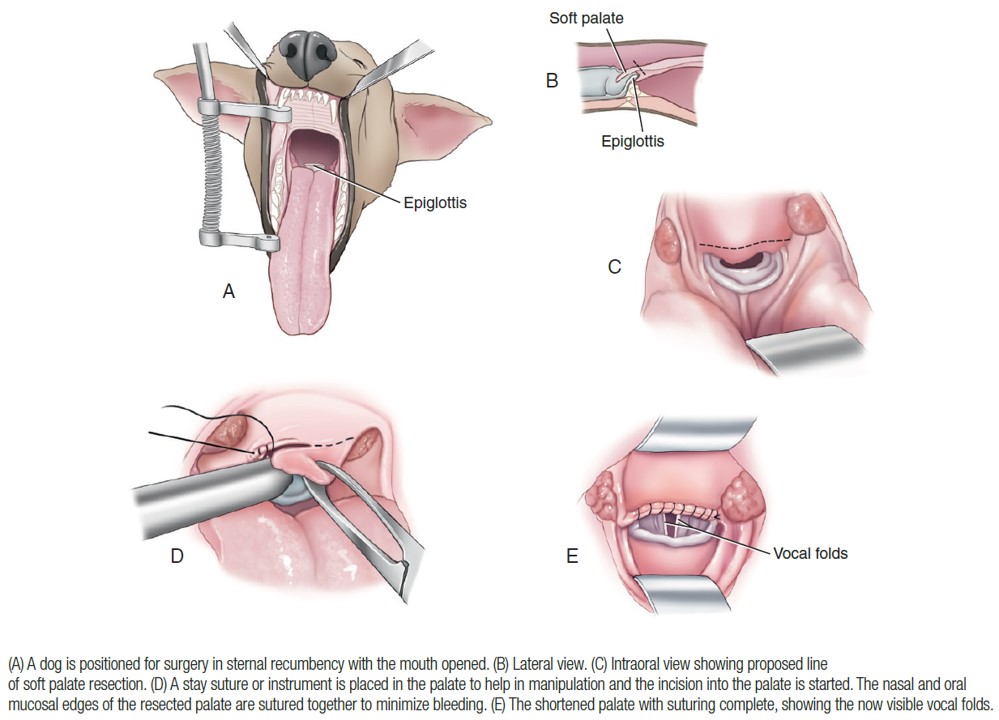
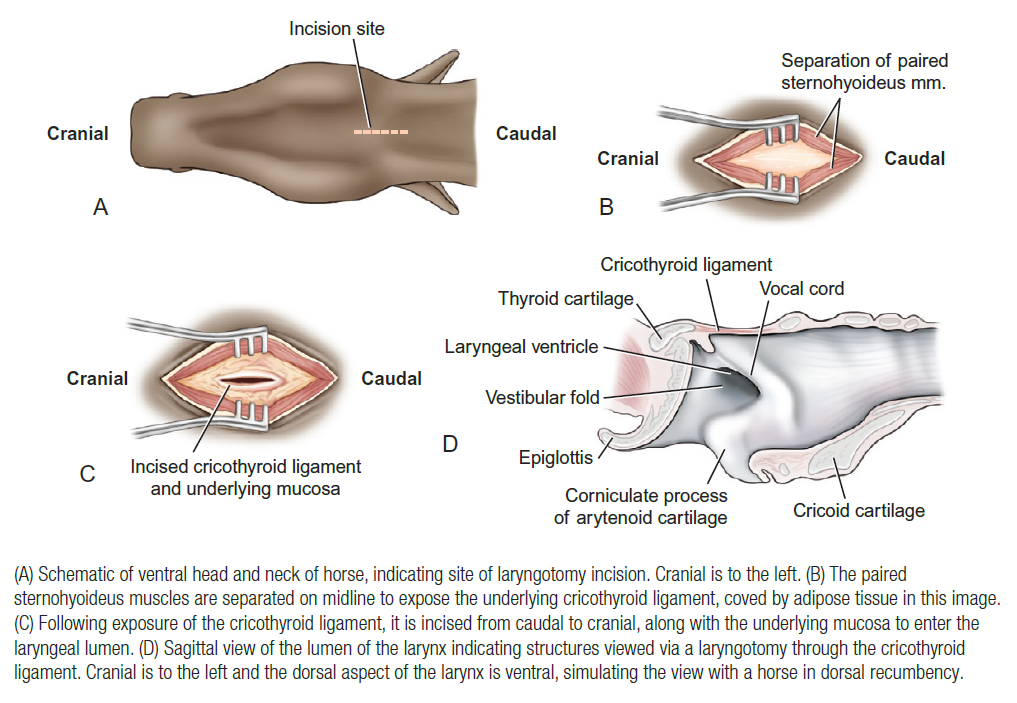
In small animal surgery a “ventriculocordectomy” is a resection of the vocal folds, also referred to as debarking or devocalization when done for this reason (the ethical considerations behind doing such a surgery to reduce a dog’s vocalization is another topic of conversation and the AVMA has a policy statement that is worth a read). Vocal folds may be resected as part of the treatment for laryngeal paralysis. Regardless of reason, the vocal folds are approached via the oral cavity or through a laryngotomy. The laryngotomy is performed by incising the cricothyroid ligament and then extending the incision cranially into the thyroid cartilage as needed for appropriate access.
Clinical application – brachycephalic obstructive airway syndrome (BOAS)
Cavity of the larynx (Cavum laryngis)
Observe: Read the following description and identify the bolded features.
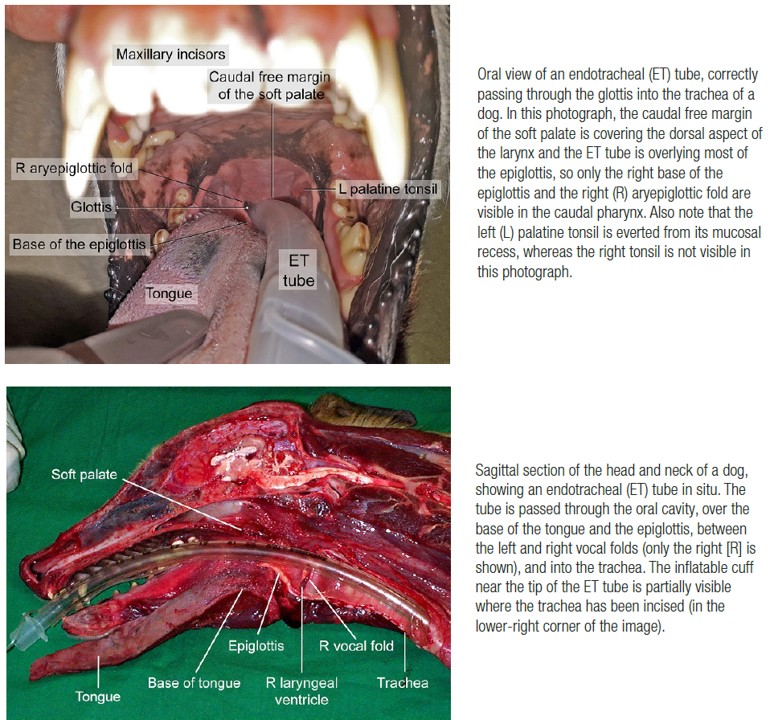
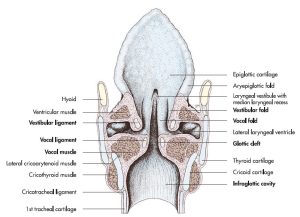
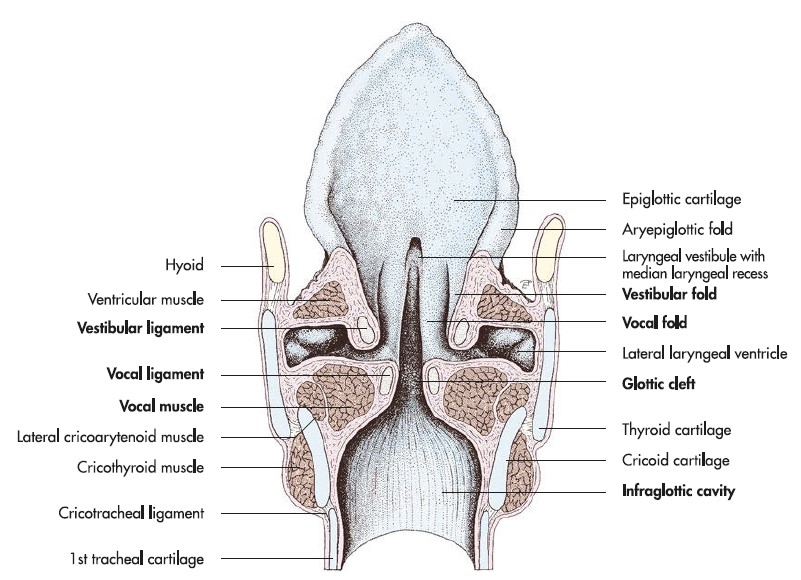
The lumen of the larynx is subdivided into an entrance, a vestibule, the glottis, and the infraglottic cavity. The entrance (aditus laryngis) is bound by the epiglottis, the aryepiglottic fold and the corniculate processes of the arytenoid cartilage (in cat, arytenoid cartilages). The vestibule (vestibulum laryngis) is just inside the entrance of the larynx, between it and the vocal folds (think back to the vestibule of the nasal cavity being just inside the entrance i.e. once through the nostrils). The glottis is the ‘voice box’ or vocal apparatus at the approximate center of the larynx, defined as a space and the structures that form the boundaries of that space. The structures include the arytenoid cartilages and the vocal folds, and the space bound by these structures is the rima glottidis or glottic cleft. The glottis represents the narrowest point of the pathway through the larynx and at this site, the size and shape of the air passageway can be altered by muscular activity. When selecting an endotracheal tube, the size of the tube (its outside diameter) is limited to the maximum width of the glottis. Caudal to the glottis is the infraglottic cavity (cavum infraglotticum) which is then continued by the trachea.
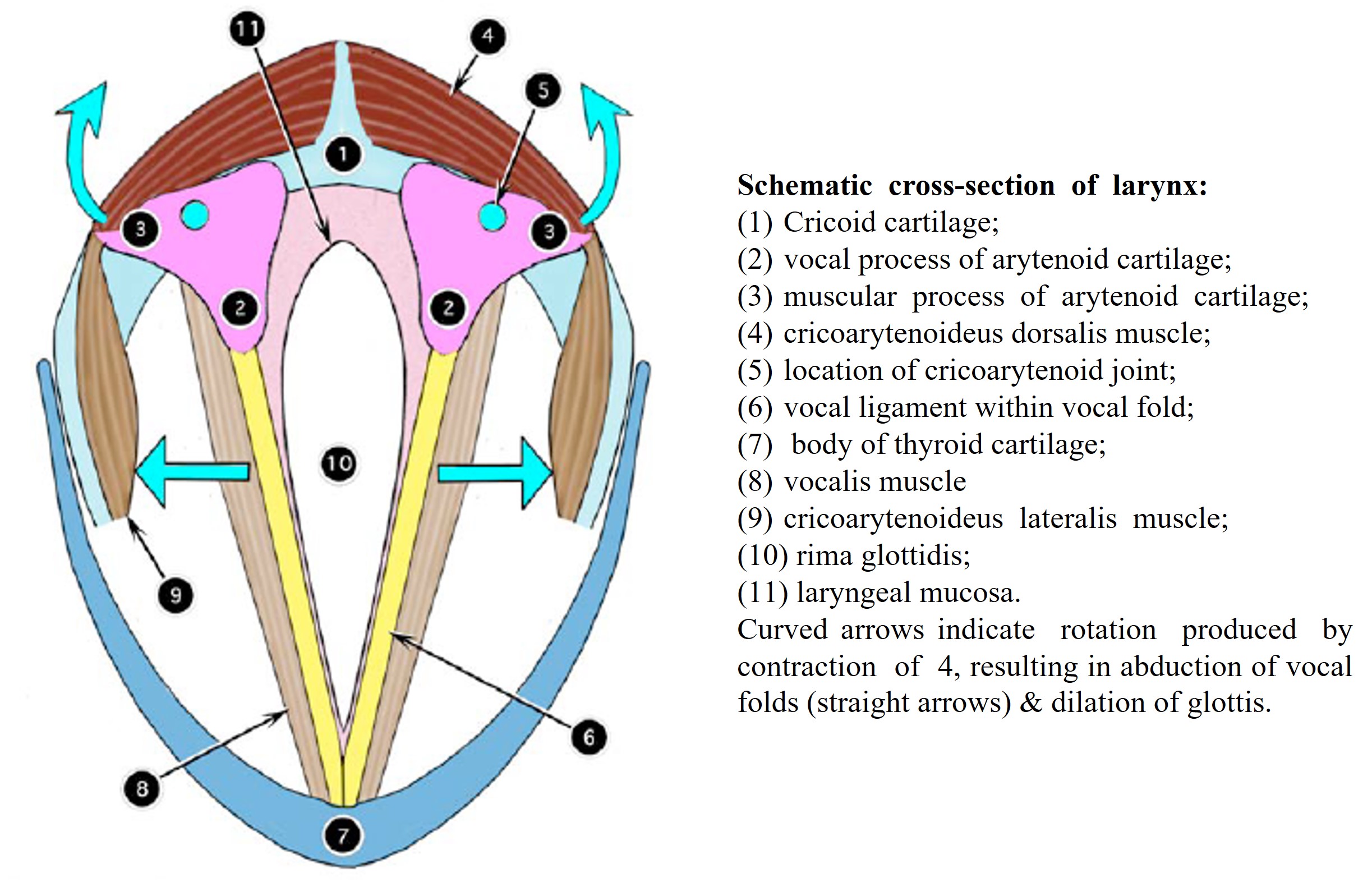
-
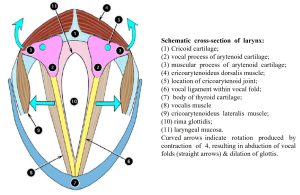
- Schematic cross section of the larynx. 2
Muscles of the larynx (Musculi laryngis)
Observe: Identify the two bolded muscles of the larynx on cadavers and on wet and plastinated prosections of the larynx. Know the attachments and function and innervation of the cricoarytenoideus dorsalis m.
The larynx has extrinsic and intrinsic muscles. Extrinsic muscles have an attachment to a laryngeal cartilage and an attachment elsewhere in the body e.g. sternothyroideus m., cricopharyngeus m. The seven intrinsic muscles have both attachments to cartilages of the larynx. The intrinsic muscles are innervated by branches of the vagus nerve. The cranial laryngeal n. innervates the cricothyroideus m. (see next paragraph) and the caudal laryngeal n. (the terminal nerve of the recurrent laryngeal n.) supplies all other intrinsic muscles – recall these nerves from our study of the Nervous System.
The cricothyroideus m. lies ventral to the insertion of the sternothyroideus muscle and passes on the lateral surface of the larynx from the cricoid cartilage to the thyroid lamina. It tenses the vocal fold indirectly by drawing the ventral parts of the cricoid and thyroid cartilages together.
The cricoarytenoideus dorsalis (CAD) m. arises from the dorsolateral surface of the cricoid cartilage and inserts on the muscular process of the arytenoid cartilage. It rotates the arytenoid so that the vocal process moves laterally, opening the glottis. It is the only laryngeal muscle that functions primarily to open the glottis. The CAD m. is innervated by the caudal laryngeal n. Dysfunction of the CAD m. leads to an inability to open the glottis. See the Clinical Application box.
FYI: The cricoarytenoideus lateralis m. arises from the lateral surface of the cricoid cartilage and inserts on the arytenoid cartilage muscular process between the cricoarytenoideus dorsalis m. and the vocalis m. It acts to close the glottis by pivoting the arytenoid cartilage inward and thus moving the vocal process medially. The thyroarytenoideus m. is the parent muscle mass that gives rise to the vocalis m. medially and ventricularis m. rostrally. It arises along the internal midline of the thyroid cartilage and inserts on the arytenoid cartilage. Its function is to relax the vocal fold and to constrict the glottis. The vocalis m., as a medial division of the thyroarytenoid muscle, arises on the internal midline of the thyroid cartilage and inserts on the vocal process of the arytenoid cartilage. The vocalis m. draws the arytenoid cartilage ventrally, thus relaxing the vocal fold. The ventricularis m., in the dog, has shifted its origin cranially to arise from the cuneiform process of the arytenoid cartilage. The muscle extends dorsally to insert on the interarytenoid cartilage, meeting its opposite partner on dorsal midline. The ventricularis m. constricts the glottis and dilates the laryngeal ventricle. The arytenoideus transversus m. passes from the muscular process of the arytenoid cartilage to insert on the interarytenoid cartilage, adjacent the ventricularis m. It also functions to constrict the glottis.
-
- Intrinsic musculature of larynx of the cat, lateral view with window in thyroid cartilage. 4
-
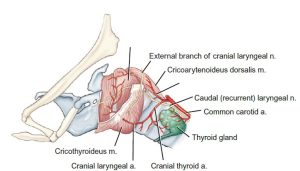
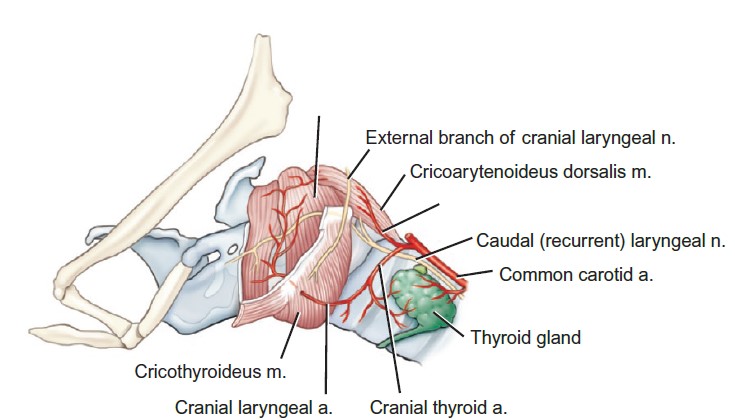
- Schematic of laryngeal vasculature and innervation of the horse as viewed from the left side. 9
Clinical Application – larynx and laryngeal paralysis
The caudal laryngeal nerves (the termination of the recurrent laryngeal nerves, which branched off the vagus n. in the thorax) innervate the left and right cricoarytenoideus dorsalis mm. Dysfunction of one or both of these nerves, and subsequent failure of one or both of the cricoarytenoideus dorsalis mm. to abduct the glottis, leads to a clinical condition called laryngeal paralysis (commonly referred to as “LarPar” in small animal medicine). Unilateral plegia or paralysis is most common (ie only one side is affected, while the other side functions as normal), but it is possible to have bilateral plegia or paralysis. Because the glottis cannot be opened to its normal extent, the animal breathes through a restricted airway. This causes increased respiratory effort, stridor (high-pitched upper respiratory sounds), exercise intolerance, and decreased ability to dissipate heat.
Anti-inflammatory medications may be administered to reduce the swelling of secondary inflammation, in an effort to partially widen the glottic cleft. However, the definitive treatment for the condition is a tie-back surgery, whereby the arytenoid cartilage is surgically abducted (using a suture prosthesis that simulates the action of the CAD m.) to open the glottis. Because the airway is permanently opened by this procedure, a complication is aspiration pneumonia (food enters the airway and causes infection in the lungs).
Horses are also diagnosed with laryngeal hemiplegia or paralysis and are called “roarers” due to their increased breathing sounds during exercise (see Ungulate section below).
Trachea and revisit of other neck structures
Observe: For this next section we are focused on identify the trachea and be sure to do so in the cadaver and on prosections. While in the region we can touch back on structures already considered and preempt a few to come in the Alimentary System.
The trachea is the connecting airway between the larynx and the lungs, subdivided into cervical and thoracic parts. It is composed of a C-shaped hyaline tracheal cartilages. The number of cartilages varies within and between species. In the cat the range maybe 38-43, and in the dog 42-46 cartilages are described. Cartilages are open dorsally, and the space is bridged by the trachealis m. (smooth muscle), attaching to the superficial surface of the cartilages (in ungulates the trachealis m. is attached to the deep surface of the cartilages). Fibroelastic annular ligaments bind one tracheal cartilage to the next, and allow for considerable flexing and extending of the tube. At its thoracic caudal end the trachea bifurcates into the left and right principle bronchi. The internally-located crest of the partition at the site of bifurcation is called the tracheal carina (to be seen in a future lab, and this feature is an imaging landmark).
FYI (to be studied in the Alimentary System): The cervical portion of the esophagus extends from the laryngopharynx to the thoracic portion of the esophagus at the thoracic inlet. It begins opposite the middle of the axis (C2) dorsally and opposite the caudal border of the cricoid cartilage ventrally. A plicated ridge of mucosa, the pharyngoesophageal limen, marks the boundary between the laryngopharynx and the esophagus. The esophagus is closely related to the dorsal and dorsolateral tracheal surface. From its origin it inclines to the left, so that at the thoracic inlet it usually lies to the left of the trachea.
FYI – revisit from Cardiovascular System: The thyroid gland is plum-colored and usually consists of two separate lobes lying lateral to the first five tracheal rings. Occasionally, a ventrally connecting isthmus is present. There are two parathyroid glands associated with each thyroid lobe. They are small, light-colored, spherical bodies (like a grain of rice). The external parathyroid most commonly lies in the fascia at the cranial pole of the thyroid lobe. It may be entirely separate from the thyroid tissue or embedded in the cranial pole of the thyroid external to its capsule. The internal parathyroid lies deep to the thyroid capsule on the medial aspect of the lobe. Occasionally, it is embedded in the parenchyma of the thyroid and is difficult to locate. The location of these glands is subject to variation.
-

- Transverse section of the trachea of the different domestic species. 7
Clinical application – trachea and tracheal surgery
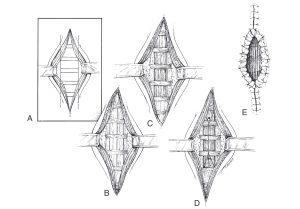
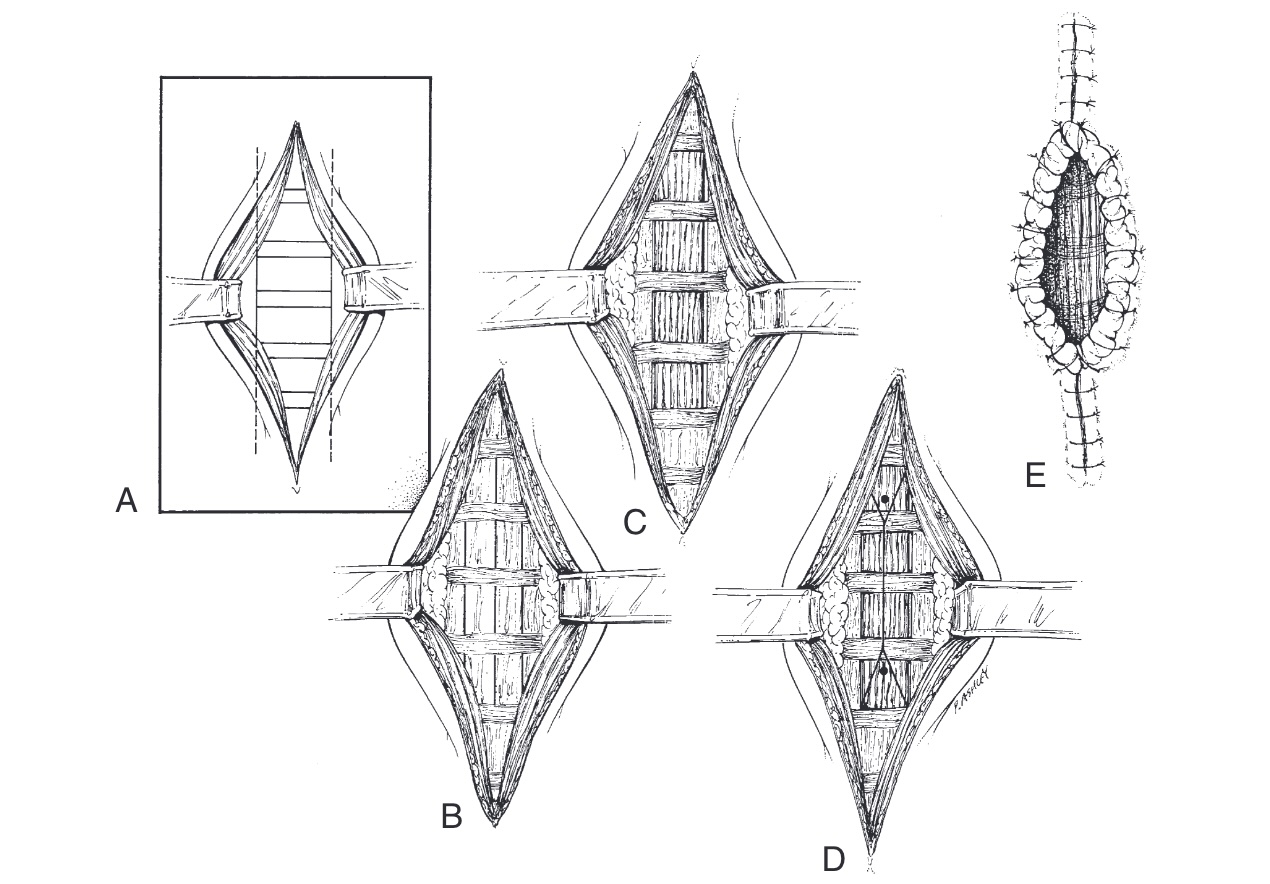
-
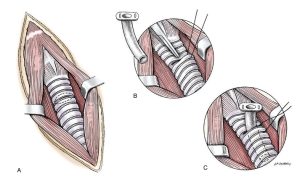
- Surgical steps for a temporary tracheostomy in a dog.29

-
- Surgical steps for a permanent tracheostomy in a dog.29
Comparative Ungulate Anatomy
Larynx, laryngopharynx and revisit to the nasopharynx
The anatomy of the larynx and laryngopharynx of the ungulates follows the standard blue-print, with a few comparative species distinctions. The nasopharynx returns to the story to complete the picture.
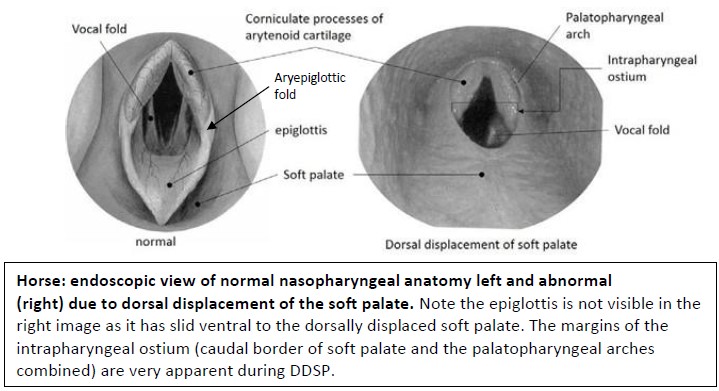
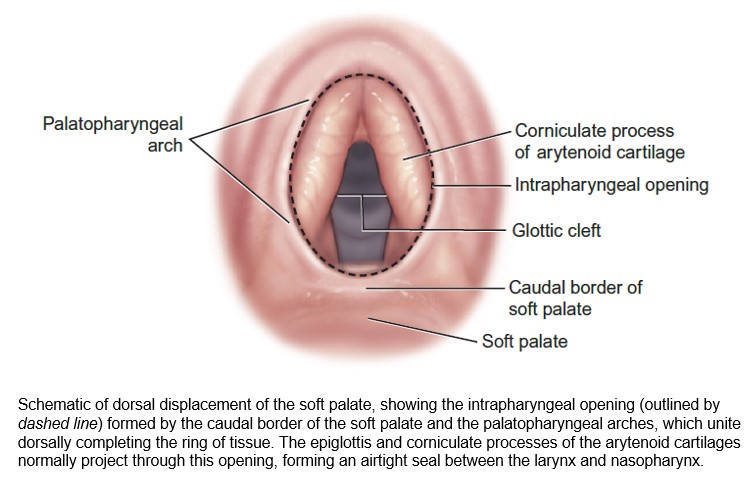
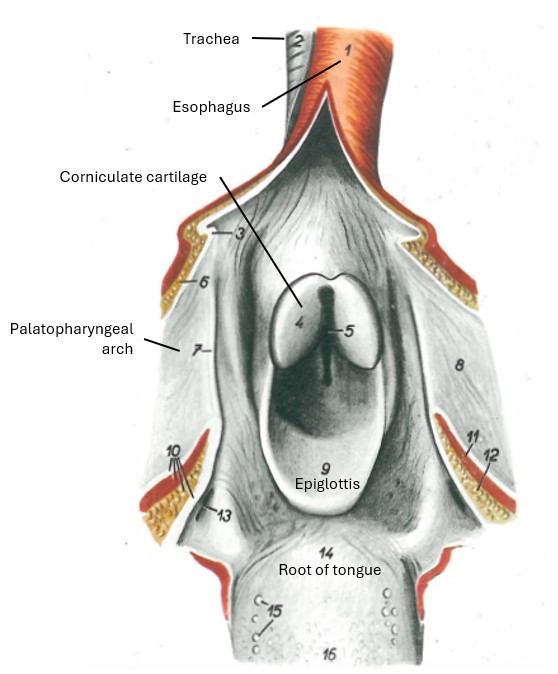
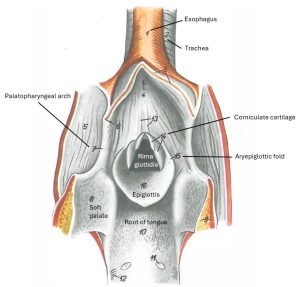
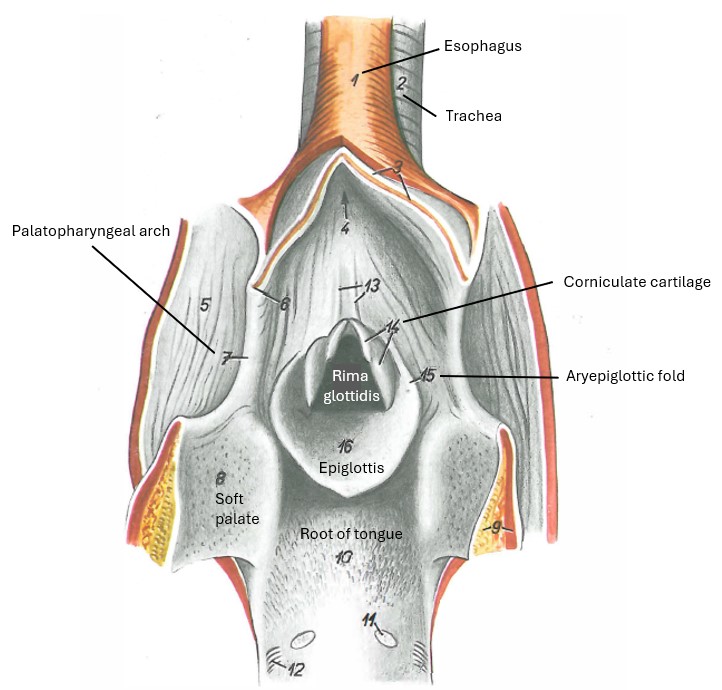
As previously stated in Lab 1A, the nasopharynx ends caudally at the palatopharyngeal arches and the caudal border of the soft palate. The arches and the soft palate form a complete ring of soft tissue, creating an opening between the space of the nasopharynx and the space of the laryngopharynx. This opening is called the intrapharyngeal ostium . Importantly, in the normal horse, the rostral aspect of the larynx, i.e. the epiglottis and corniculate processes of the arytenoid cartilages, projects through this opening into the nasopharynx space. This ‘interlocking’ of the larynx with the nasopharynx creates an effective seal between the two structures and explains why the horse is an obligate nasal breather, at rest, and during exercise. Horses do not/can not breath through their mouth as a normal function. The only time the larynx moves out of the intrapharyngeal ostium is during normal swallowing or in certain pathological conditions of the airway. Even during these pathological conditions the horse continues to breathe through its nose, but the flow of air into and out of the larynx will be less streamlined (and so we hear abnormal airway sounds and the horse has exercise intolerance when such conditions arise).
-
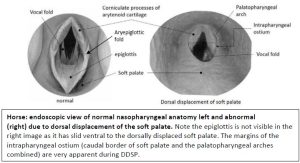
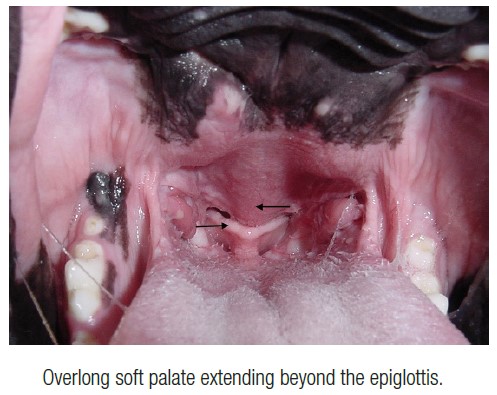
- Horse: endoscopic view of normal nasopharyngeal anatomy left and abnormal (right) due to dorsal displacement of the soft palate.
-
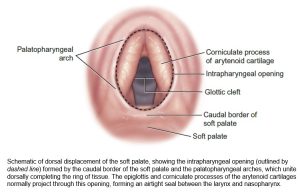
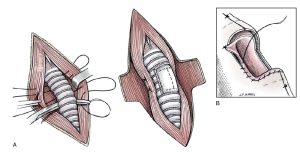
- Dorsal displacement of the soft palate, showing the intrapharyngeal ostium. 9
-
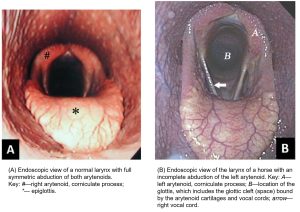
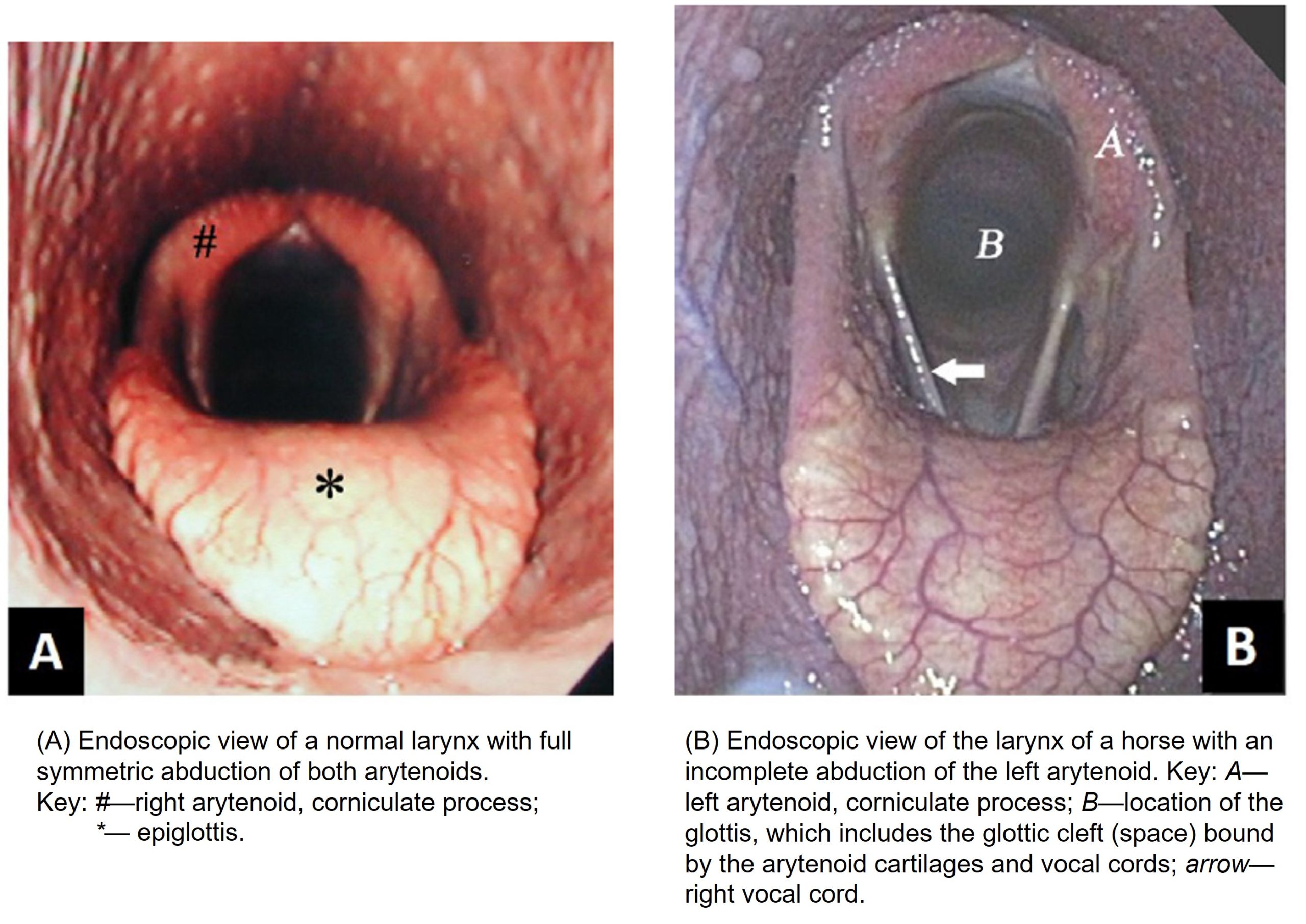
- Normal and abnormal opening of the glottis. 9
In ruminants and the pig (and carnivores) there is a relatively ‘loose’ relationship between the rostral larynx and the nasopharynx and the larynx more freely moves in or out of the intrapharyngeal ostium, not just when swallowing occurs. Therefore, air can be effectively directed into the larynx via the nose or the mouth. Typically nasal flow is the norm, however the heat-stressed carnivore, ruminant and pig, can all pant (i.e. mouth breath) as a physiological response.
Given the athletic use of the horse, the equine larynx is frequently evaluated for causes of abnormal airway noise and exercise intolerance. Endoscopic examination of the equine upper respiratory tract is routine and one of the most sensitive and specific methods of diagnosis. A clear understanding of the normal endoscopic appearance of the anatomy is necessary to detect abnormal, which may only be a subtle asymmetry of structures.
Observe: Retrieve models and prosections of the ungulate species. Examine both halves of sectioned cadavers on their medial side and refer to wet and dry specimens for comparative study of the larynx. Be sure to understand the relationship of the larynx to the nasopharynx and laryngopharynx. Distinguish why the horse is an obligate nasal breather, whereas our other domestic species being studied are not.
Equine larynx – comparative notes
The cuneiform process (part of the arytenoid cartilage in the dog) has migrated rostrally to become a process extending from the epiglottis (it need not be identified). The aryepiglottic fold is prominent. The vestibular and vocal folds and the laryngeal ventricle are readily seen. The thyroid cartilage has a deep caudal thyroid notch, which results in a relatively long cricothyroid ligament filling the space. The attachments, location, and function of the CAD m., the caudal laryngeal n. (clinically, we often simply refer to its parent nerve, the recurrent laryngeal n.), the cricoarytenoid joint, and the action of the preceding linked structures on the glottis, is highly clinically relevant in the horse.
-
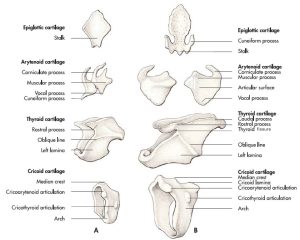
- Laryngeal cartilages of the dog (A) and the horse (B). 7
-
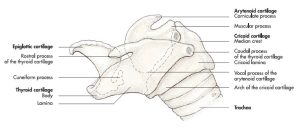
- Laryngeal cartilages of the horse. 7
-
- Dorsal section of the larynx of the horse. 7
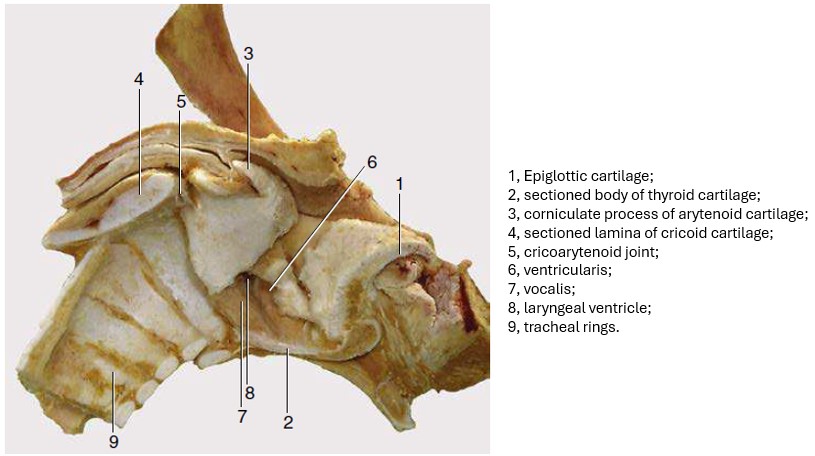
-
- Median section of the equine larynx. 8
-
- Median section of the equine larynx after removal of the mucosa. 8
-
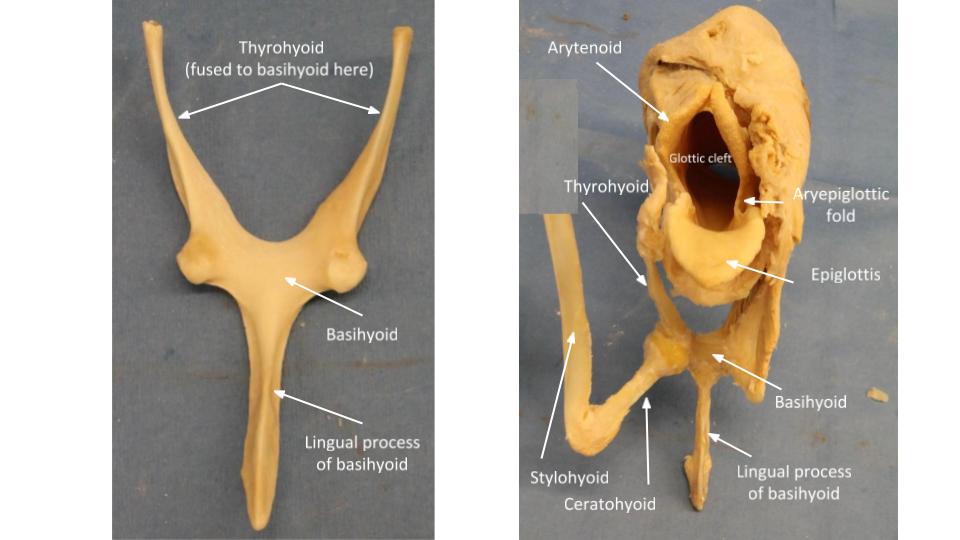
- Horse larynx

-
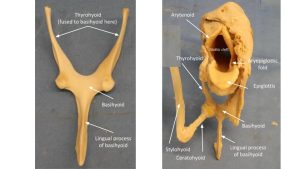
- Horse lingual process of basihyoid
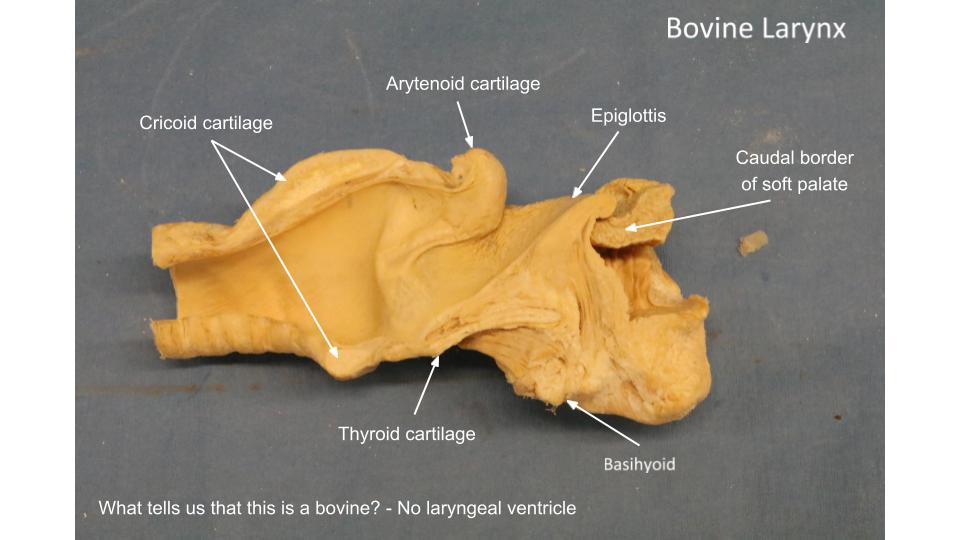
Ruminant larynx – comparative notes
Laryngeal ventricles and vestibular folds are absent in the ruminant. The epiglottis has a more rounded shape.
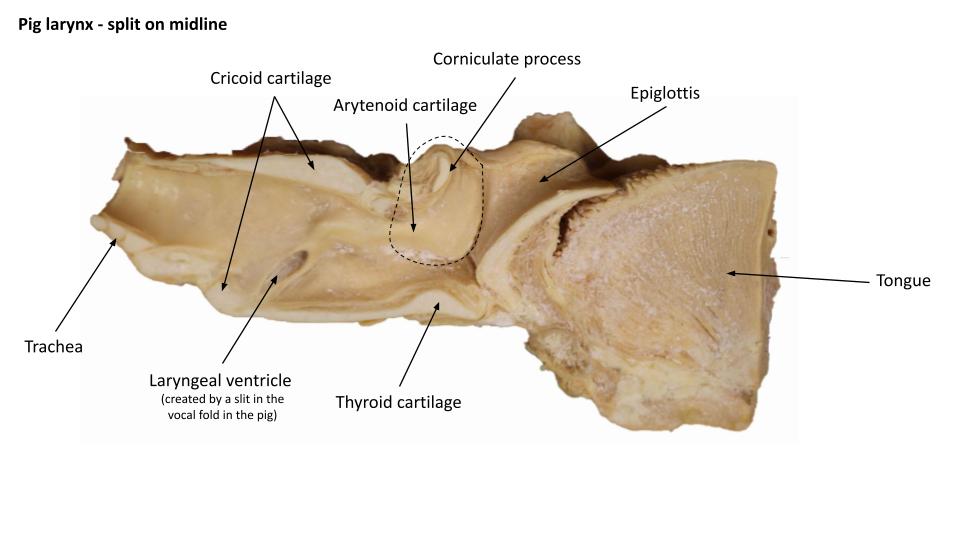
Pig larynx – comparative notes
Pigs lack a vestibular fold, however laryngeal ventricles are present. The entrance to the ventricle is created by a slit in the vocal fold. The arytenoid cartilages have large corniculate processes and they are fused on midline dorsally. On the lateral side of each corniculate process is an obvious semilunar appendage, that creates the appearance of miniature corniculate processes being present along with the normal sized version.
-
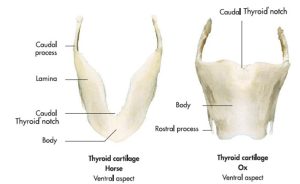
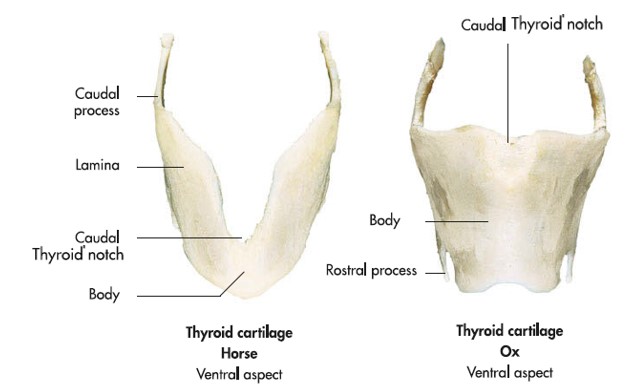
- Thyroid cartilages of a horse and an ox. 7
-
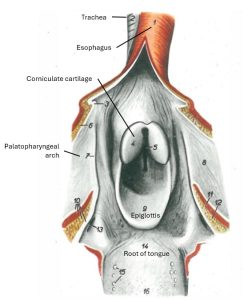
- Larynx of the ox. 11
-

- Ruminant larynx
-
- Larynx of the pig.
-
- Pig larynx
Clinical application – recurrent laryngeal neuropathy and laryngeal hemiplegia
Dysfunction of the recurrent laryngeal n. (known as recurrent laryngeal neuropathy or RLN) causes laryngeal hemiplegia (LHP), a common condition diagnosed in the performance horse, with a very strong predilection to the left side (why might this be the case?). If the nerve is not working, the CAD m. is not able to contract, and the arytenoid cartilage cannot be rotated at the cricoarytenoid joint, to abduct (open) the glottic cleft of the glottis. Due to the partially obstructed airway and consequent airway sounds made at exercise, the horse with LHP is known as a “roarer”; similar to the “LarPar” of carnivores, a laryngoplasty (laryngeal tie-back surgery) may be indicated. Besides the laryngoplasty, ventriculocordectomy (remove the laryngeal ventricle and vocal fold), or vocal cordectomy (remove vocal fold only) are performed. This is done to further stabilize the abducted arytenoid cartilage through additional scarring (fibrosis), and to remove tissues that may potentially deviate into the lumen of the larynx during strenuous exercise, following laryngoplasty.
Clinical application – cricothyroid ligament and laryngotomy
Clinical application – aryepiglottic fold diseases
Trachea
Equine trachea – comparative notes
The horse trachea is flattened dorsoventrally and consists of 48-60 cartilages. The trachealis m. is attached to the deep side of the cartilages.
Ruminant trachea – comparative notes
The ruminant trachea consists of 48-60 cartilages and the trachealis m. is attached on the deep side of these cartilages. It is relatively oval in cross section on the live ox, whereas in the goat it is more U-shaped on cross section. The sheep has 3 regions of different cross sectional shape along the length of its trachea. The tracheal bronchus specifically supplies the right cranial lung lobe (cranial and caudal parts).
Pig trachea – comparative notes
The pig trachea is circular in cross section and has a range of 32-36 cartilages. The ends of the incomplete cartilaginous rings overlap each other. The trachealis m. lies on the deep surface of the cartilages. The tracheal bronchus specifically supplies the right cranial lung lobe.
-
- Transverse section of the trachea of the different domestic species. 7
Clinical application – trachea and tracheal surgery
Tracheotomy and temporary or permanent tracheostomy are relatively common procedures in the horse, and less so in the artiodactyls. The surgical principles and applied anatomy are similar to carnivores. When an emergency tracheotomy is required to establish an airway for survival, a keen understanding of the surgical anatomy is helpful. Take the time, now, to talk through the anatomy of the procedure – to the point that a standing horse or ox, struggling with dyspnea, can suddenly suck in a lungful of air with ease. As the animal realizes its air hunger is no longer, one can observe their evident deep sense of relief.
-
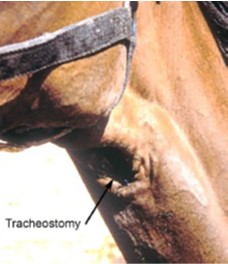
- Horse with a permanent tracheostomy. 9
-
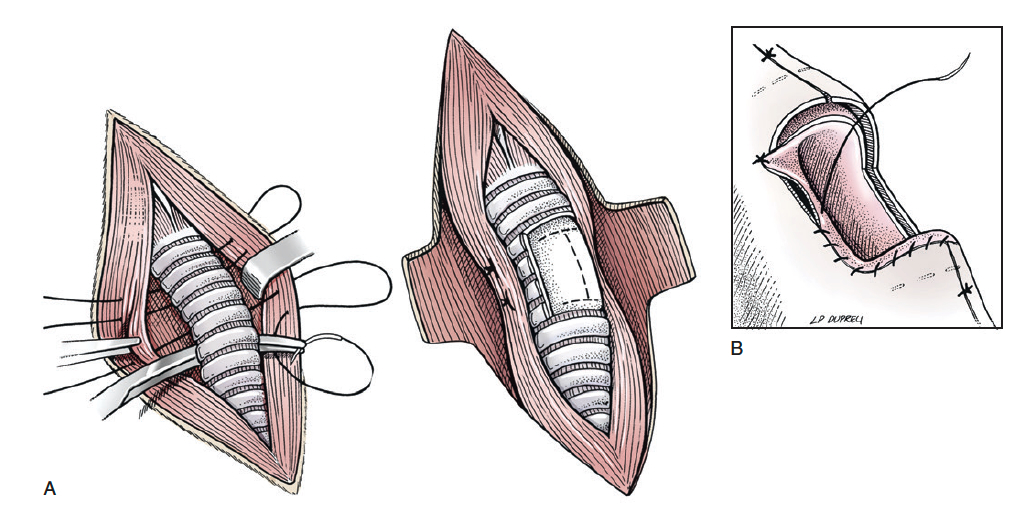
- Permanent tracheostomy surgical steps in horse. Equine Surgery 5th Ed.
Review videos
Dog larynx – 5 min
Dog larynx – 6 min, watch until 17 min (generally same information as video above)
Horse larynx – 8:30 min, watch until 10 min
Pig larynx – 2 min
2025 video:
Comparative larynges – 12 min
TERMS
| Carnivore | |
| Laryngopharynx | Larynx |
| Piriform recesses | Epiglottis |
| Aryepiglottic fold | |
| Thyroid cartilage | |
| Cricothyroid ligament | |
| Cricoid cartilage | |
| Cricoarytenoid joint – be aware of | |
| Arytenoid cartilages | |
| Trachea | Muscular process |
| Tracheal cartilages | Corniculate process (dog only) |
| Cuneiform process (dog only) | |
| Vocal process | |
| Vestibular fold (dog only) | |
| Laryngeal ventricle (dog only) | |
| Vocal fold | |
| Glottis | |
| Rima glottidis or glottic cleft | |
| Cricothyroideus m. | |
| Cricoarytenoideus dorsalis m. | |
| Caudal (recurrent) laryngeal n. (be aware of function) | |
| Ungulate | |
| Feature | Comment |
| Laryngopharynx | |
| Piriform recesses | |
| Larynx | |
| Epiglottis | |
| Aryepiglottic fold | |
| Thyroid cartilage | |
| thyroid notch | notch in ventral caudal border |
| Cricothyroid ligament | laryngotomy site |
| Cricoid cartilage | |
| Cricoarytenoid joint | be aware of function |
| Arytenoid cartilages | |
| Muscular process | |
| Corniculate process | |
| Vocal process | |
| Vestibular fold | horse |
| Laryngeal ventricle | horse, pig |
| Vocal fold | split in the pig (forming entrance to ventricle) |
| Glottis | |
| Rima glottidis or glottic cleft | |
| Cricoarytenoideus dorsalis m. | |
| Caudal (recurrent) laryngeal n. | be aware of function |
| Trachea | |
| tracheal cartilages | |