Lab 3A: Upper Respiratory Tract 3 – Ungulate Paranasal Sinuses and Equine Guttural Pouch
Learning Objectives
- Describe what a paranasal sinus is, and recall their functions
- Identify the paranasal sinuses, and their communications, of the horse and ruminant
- Describe and identify the drainage pathways of the paranasal sinuses, with an emphasis on the horse
- Associate the paranasal sinuses with clinical conditions and procedures
- Describe and identify the trephination access points to select paranasal sinuses
- Identify the guttural pouches (GPs) of the horse and their associated neurovascular, bone, muscle, and lymph node structures
- Associate and apply the normal anatomy of the guttural pouch and surrounding structures to clinical signs of diseases of the GPs
Lab Instructions:
This lab is entirely focused on the ruminant and horse, considering two regions of the upper respiratory tract that get frequent clinical attention, albeit much more so in the horse. Use prosections, wet and dry, and skulls with sculptured access to the paranasal sinuses, to explore and learn the anatomy. Due to limited numbers of specimens to study, Teams 1-12 may start with skull specimens to consider paranasal sinus anatomy, and Teams 13-25 may start with prosected head specimens of the horse to study guttural pouch anatomy. Any dissection instructions provided in this lab are for the instruction team to follow, in their preparation of the prosected head cadavers.
Horse cadaver: from the nasal cavity side, cut a rectangular window into the wall of the dorsal and ventral nasal conchae at their caudal extents to expose the dorsal and ventral conchal sinuses. Thread a zip tie through the nasomaxillary opening by gently passing it via the caudal extent of the middle nasal meatus, dorsolaterally between the walls of the dorsal and ventral nasal concha, into the caudal maxillary sinus. Leave the zip tie in place as an identifier of the nasomaxillary opening.
Paranasal sinuses – horse and ruminant
Observe: Use available skulls and prosected cadavers to identify the structures bolded in the following descriptions. A review of skull bones and features is also relevant to fully understand the paranasal sinus anatomy.
Overview
Paranasal sinuses are a complex of interconnected, air-filled chambers between outer and inner cortices of bones of the skull, and some are enclosed by nasal conchal walls. They represent a type of “pneumatization” of bone similar to that which occurs in most birds. Paranasal sinuses are extensive in the ungulates and there are important comparative differences.
In general there are four categories of sinuses, named for the bone or concha they reside in:
- Frontal
- Conchal—dorsal, middle, ventral
- Maxillary
- Sphenopalatine (or sphenoid and palatine)
The paranasal sinuses are lined with respiratory mucosa and they drain directly or indirectly into the nasal cavity. This drainage is a function of active ciliary transport and passive gravity-dependent flow. There are left and right sets of paranasal sinuses, divided on midline by a bony septum. The exception to this, in the horse, is the small sphenopalatine sinus, which has considerable individual variation and sometimes communicates with its counterpart. What purpose do paranasal sinuses serve, besides causing problems when they get congested or infected? Because of their communication with the nasal cavity, they are usually considered with the respiratory system, even though they do not have any recognized respiratory function. In essence, these sinuses allow for substantial expansion (growth) of the head, without a commensurate increase in the weight of the head. By expanding the bones through pneumatization, the head becomes larger to accommodate more “things” (viz. teeth, glands, tongue, etc.) and the sinuses provide a collapsible, ‘crumple zone’, a non-vital protective shell around the brain and other deep head structures. In other words, the sinuses allow for the head to get big and strong, without becoming so heavy that the animal could not hold it up. The sinuses also have a role in innate immune function.
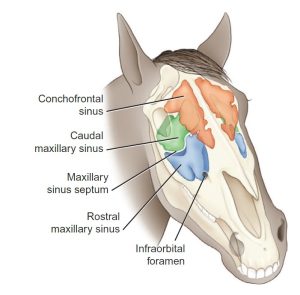
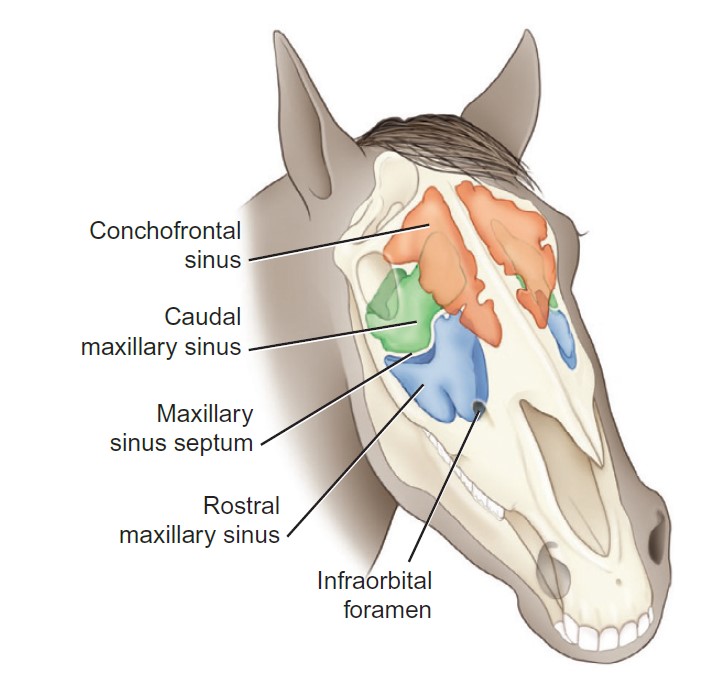
Horse paranasal sinuses
The frontal sinus is the largest of the paranasal sinuses in surface area. It is roughly triangular in shape and primarily occupies the forehead region and the area between the eyes. In the horse, at its rostromedial aspect, the frontal sinus communicates widely with the dorsal conchal sinus, and the combined sinuses are often referred to as the conchofrontal sinus. The caudal limit of the frontal sinus overlays the cranial cavity, and awareness of this anatomical relationship is critical when entering the frontal sinus, to avoid damaging the CNS. The ethmoidal conchae protrude dorsally into the floor of the frontal sinus.
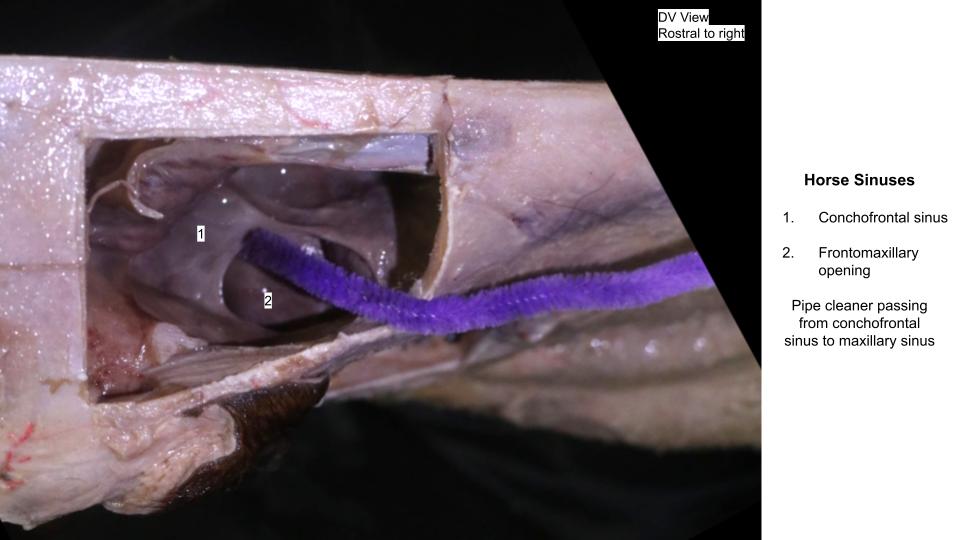
The conchofrontal sinus freely communicates with the caudal maxillary sinus through the large, ovoid frontomaxillary opening. This opening is rostrolateral to the protruding ethmoidal conchae and is typically 4–5 centimeters long and 2–3 centimeters wide.
-
- The region of the conchofrontal and caudal and rostral maxillary sinuses, which may be percussed to detect any changes in sound. 9
-

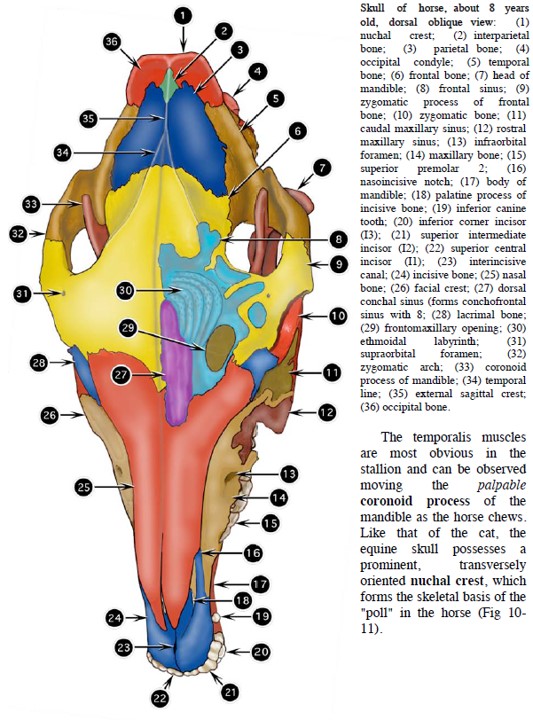
- Skull of a horse, dorsal view. 2
-

- Frontomaxillary opening
-

- Conchofrontal sinus

As mentioned, the dorsal conchal sinus represents a rostromedial extension of the frontal sinus, the two spaces more commonly referred to as the conchofrontal sinus, in the horse. A transverse conchal septum separates the dorsal conchal sinus from the scrolled, non-sinus portion of the dorsal nasal concha, continuing rostrally. The middle conchal sinus is a smaller chamber encased by the middle nasal concha (also referred to as the greater ethmoturbinate). The middle conchal sinus communicates with the caudal maxillary sinus. The ventral conchal sinus is contained within the caudal part of the ventral nasal concha, partitioned by a conchal septum from the rostral scrolled portion It communicates dorsally with the rostral maxillary sinus via the narrow conchomaxillary aperture.
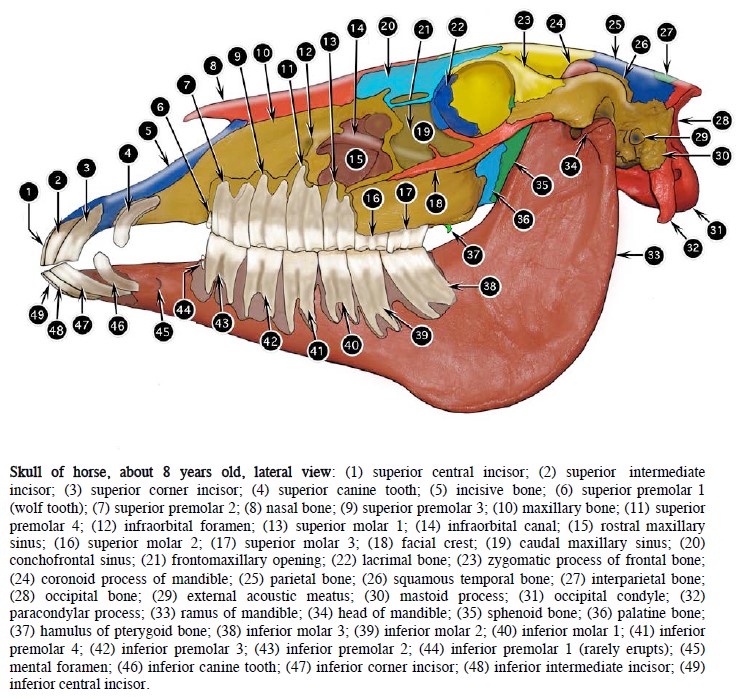
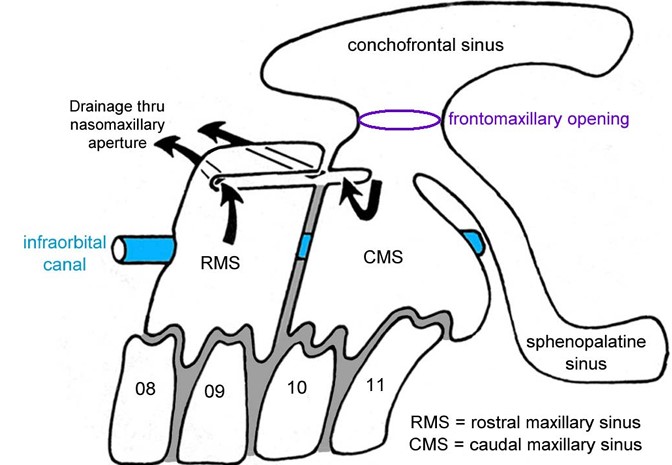
The maxillary sinus is the largest, in volume, of the paranasal sinuses. It is divided by a bony maxillary sinus septum into two chambers, the larger caudal maxillary sinus and the smaller rostral maxillary sinus. The septum runs obliquely in a medial, caudal, and dorsal direction from its lateral margin, which is usually located at about the level of the maxillary second molar tooth (Triadan 110/210). The septum is very thin and rounded at its dorsal extent, and is readily seen on sinoscopy in the normal horse. This thin, dorsal expansion of the maxillary septum is termed the maxillary septal bulla. The osseous infraorbital canal is an important feature passing through the maxillary sinus. The canal encloses the infraorbital nerve and vessels along their rostrally directed path towards their exit at the infraorbital foramen. In the caudal maxillary sinus, the infraorbital canal partially divides the chamber into medial and lateral compartments. In the rostral maxillary sinus the infraorbital canal and its supporting bone plate form the medial boundary of that sinus. On the other side of this boundary, ie medial to it, is the space of the ventral conchal sinus. These two sinuses connect over the top of the infraorbital canal, through the narrow conchomaxillary opening.
-
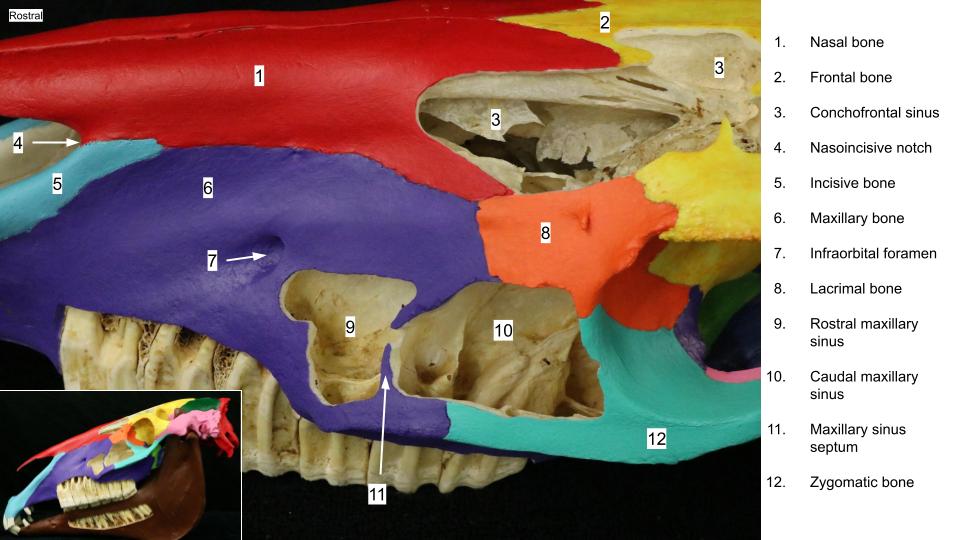
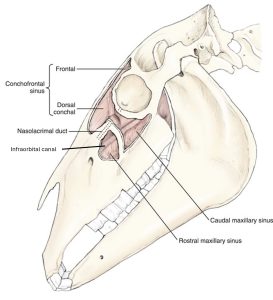
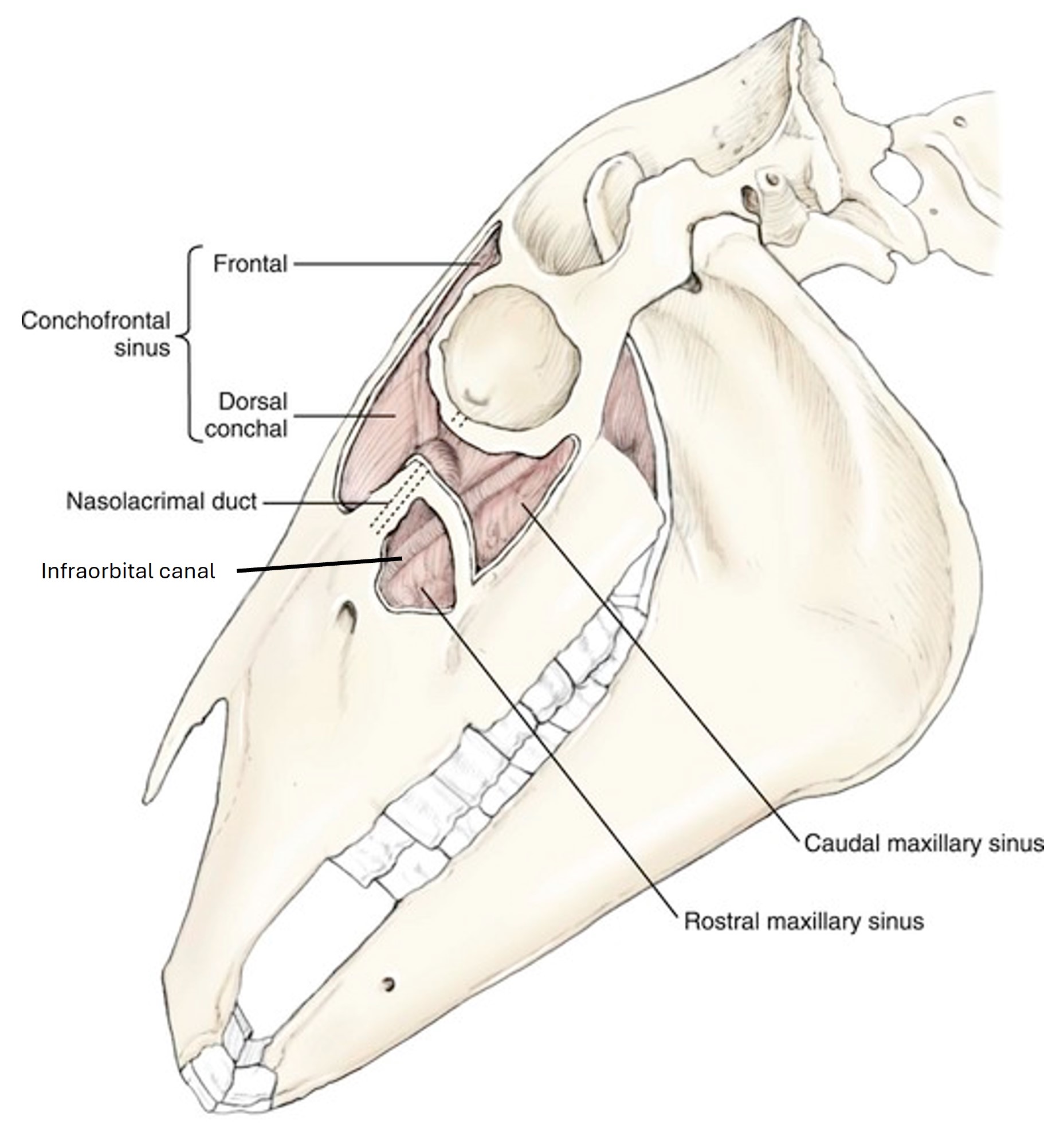
- Skull of a horse. 2
-
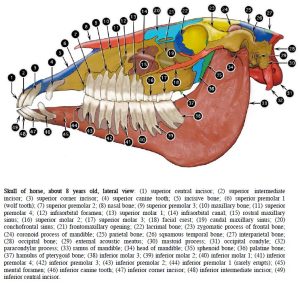
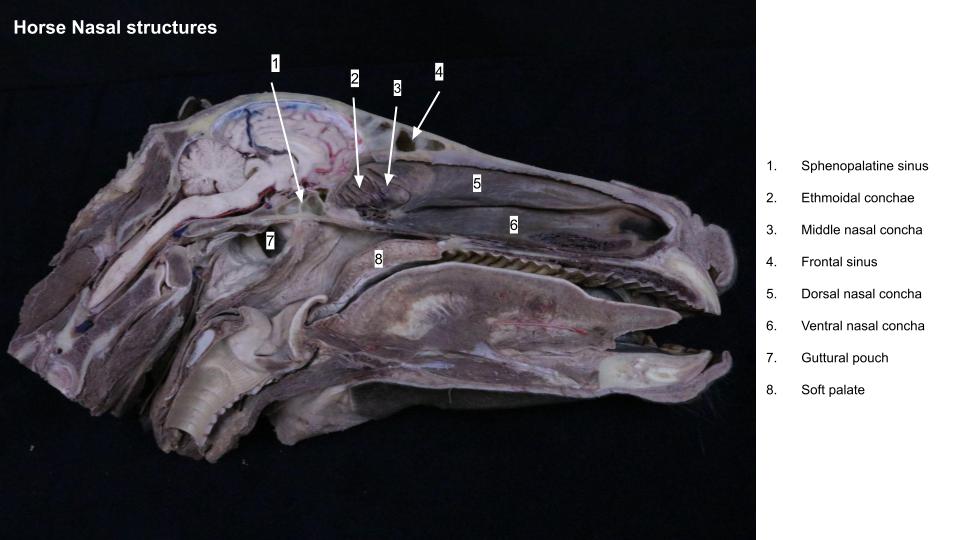
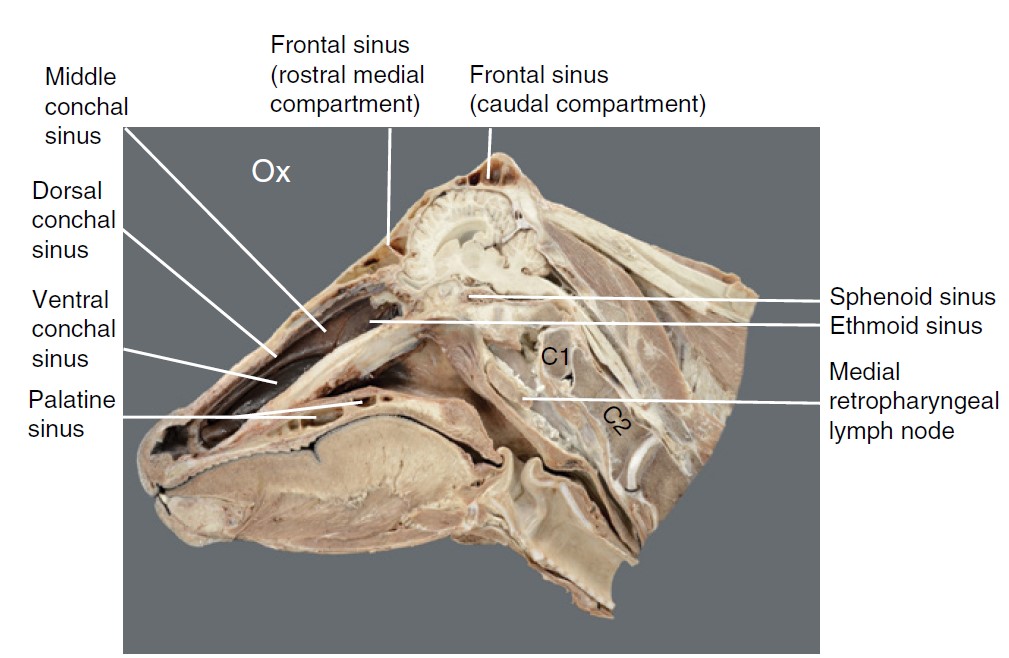
- Sagittal section of horse head. 2
-
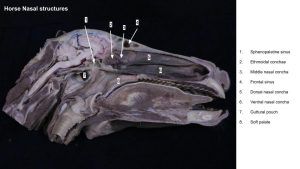
- Horse nasal structures
Clinical application – IO canal and nerve injury in sinus disease
Space-occupying masses within or extending into the maxillary sinus may injure the infraorbital canal and cause its resorption, thereby also exposing or destroying the infraorbital nerve and vessels.
-
- The infraorbital canal bisects the maxillary sinus. 31
The rostral and caudal maxillary sinuses each communicate with the middle nasal meatus of the nasal cavity through the shared, slit-like nasomaxillary opening. This is the final outflow path for paranasal sinus secretions. The caudal maxillary sinus communicates dorsally with the conchofrontal sinus via the previously mentioned frontomaxillary opening. Caudomedially, the caudal maxillary sinus communicates with the sphenopalatine sinus, and medially it communicates with the middle conchal sinus. Dental apices and reserve crowns of the last 3-4 maxillary cheek teeth, wrapped in alveolar bone, project into the maxillary sinus. In the young animal much of the maxillary sinus space is occupied by these dental structures. As the animal matures and ages the sinus space expands with skull growth and as teeth erupt and wear.
-
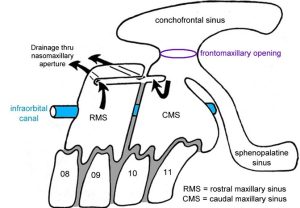
- A schematic illustration of equine paranasal sinuses. 32
-
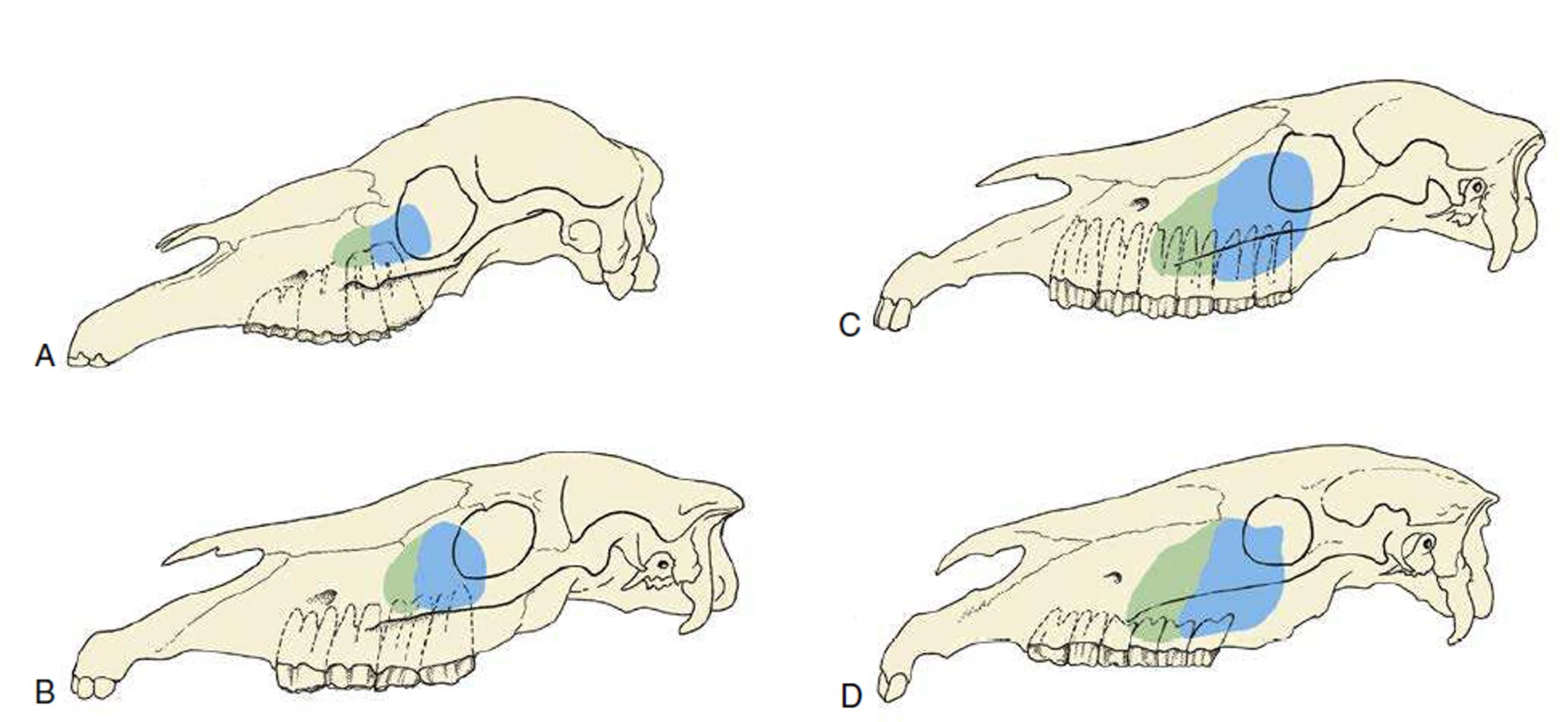
- Projection of the maxillary sinuses at various ages. In older horses the cheek teeth are more rostrally placed. (A) 1 month. (B) 1 year. (C) 4 to 6 years. (D) Older than 12 years. 8
-
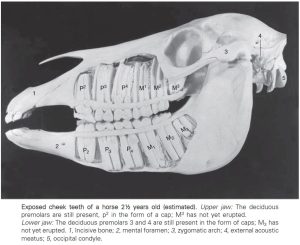
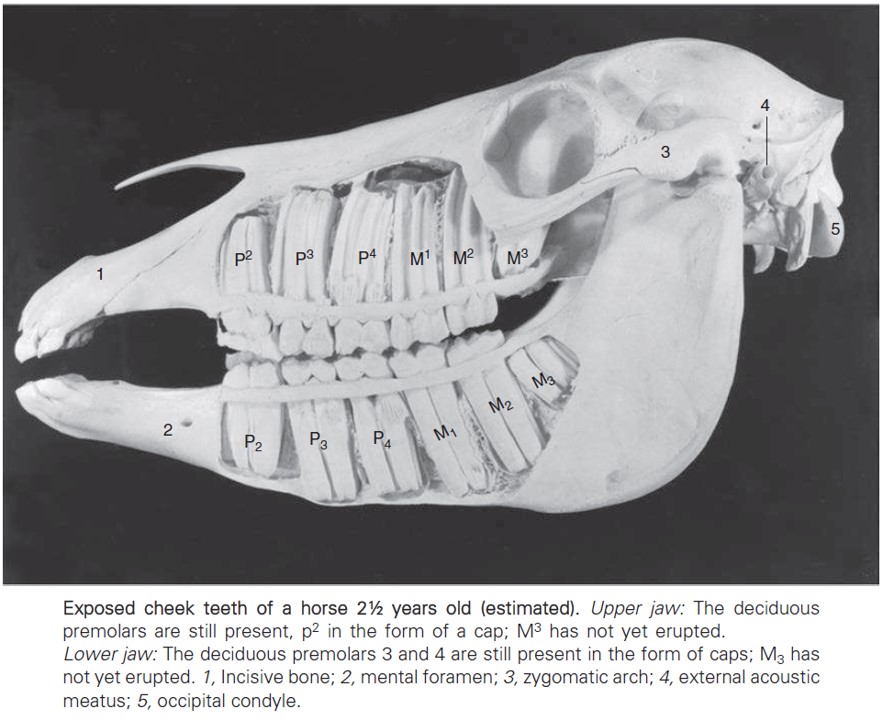
- Exposed cheek teeth of a horse 2½ years old. 8
-

- The apices (roots) of cheek teeth are prominent in the maxillary sinuses of younger horses.

On the external skull the surgical boundaries of the maxillary sinus are outlined as follows:
- Ventrally – facial crest
- Rostrally – line drawn from rostral end of facial crest to infraorbital foramen
- Dorsally – line drawn from infraorbital foramen to medial canthus of the eye
- Caudally – the tangential edge of the ventral bony orbital rim, drawn from the dorsal to the ventral boundary.
The external dorsal margin of the maxillary sinus is approximately along the pathway of the lacrimal canal – the osseous canal that protects the nasolacrimal duct as it traverses from the eye to the rostral nasal cavity.
The small sphenoid and palatine sinuses in the horse frequently communicate with each other and therefore, they are referred to as the sphenopalatine sinus. This sinus is located deep within the skull, caudoventral to the ethmoidal conchae and ventral to the rostral portion of the cranial vault. Cranial nerves and vessels pass in canals around the sphenopalatine sinus. Unlike the other paranasal sinuses, a median bony septum separating left and right sides is not a consistent finding. The sphenopalatine sinus communicates with the caudal maxillary sinus medial to the infraorbital canal. Surgical access is relatively technically difficult and limited.
-
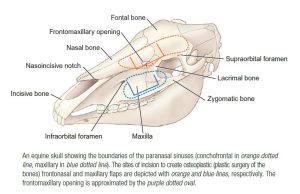
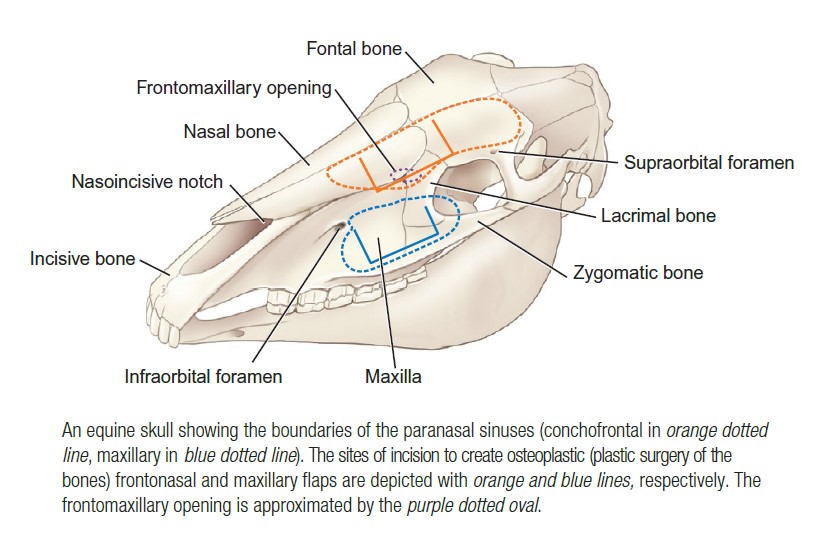
- Surgical incisions into the horse sinuses. 9
-
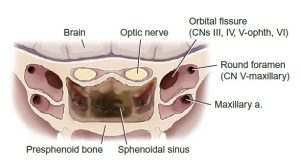
- The equine skull sectioned transversely through the sphenopalatine sinuses. 9
Clinical relevance – paranasal sinus diseases
Diseases of the paranasal sinuses are common in the horse and can be primary or secondary. Primary diseases included sinus cyst, progressive ethmoid hematoma, neoplasia and infection (primary sinusitis). Sinus cysts and neoplasia, with disease progression, may result in facial distortion as the mass expands beyond the confines of the sinus space it is growing in. Secondary sinusitis may occur subsequent to dental disease, because the apices (tooth roots) of the upper cheek teeth extend into the space of the maxillary sinuses. A tooth root infection can cause alveolar destruction and readily spread into the sinus space. The first clinical sign noted for dental disease in the upper cheek teeth may be malodorous, purulent nasal discharge, due to the drainage of the infected sinus exudate into the nasal cavity.
-

- Copious quantities of purulent exudate flowing from a nasofrontal (=conchofrontal) bone flap osteotomy in a horse with chronic sinus empyema. 33

-

- The large swelling of the left side of this 8-year-old horse’s rostral maxillary area (arrows) is the result of bone remodeling in response to an expanding cyst within the maxillary sinuses. 33

Clinical relevance – surgical access to the sinuses
Surgical access to the paranasal sinuses is routine – to inspect via sinoscopy, to explore, to obtain specimens of tissue and fluid for diagnosis, and to treat (debride, remove masses, help repel teeth, place indwelling lavage catheters). Access is created by trephination, or by performing a sinusotomy (aka a ‘bone flap’). Trephination is the process of creating a circular hole into the sinus using a drilling device called a trephine.
-

- Trephining the conchofrontal sinus.

-

- A sinusotomy (‘bone flap’) of the right conchofrontal sinus. A green-red mass is visible.

Book chapter: Dental Disease and Sinusitis – Dr. Callie Fogle & Dr. Mathew Gerard
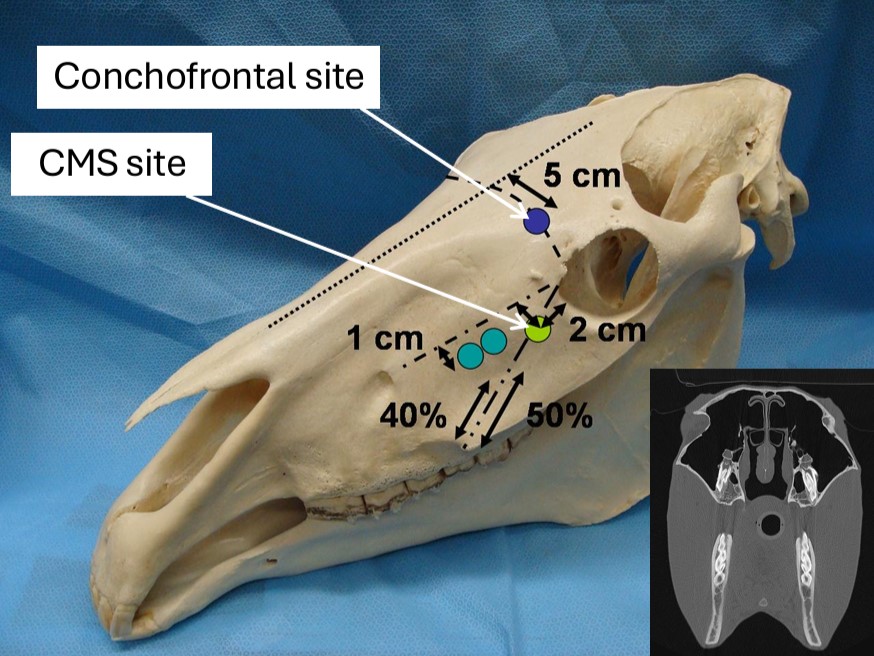
Clinical application – conchofrontal and caudal maxillary sinus trephination sites
Trephination of the equine conchofrontal sinus: draw an imaginary line connecting left and right medial canthi (the medial angle or corner of the eye). On the side to enter, mark the drill spot on the ‘canthi line’ at ~5 cm from dorsal midline (it is usually about halfway between midline and canthus). Trephining at this location provides full access to the conchofrontal sinus and, via the frontomaxillary opening, and endoscope and instruments can be passed into the caudal maxillary sinus. Further manipulations are also possible.
Trephination of the equine maxillary sinus: entry sites for the caudal and rostral maxillary sinuses are described. To enter the caudal maxillary sinus, the location is marked as 2 cm rostral to the orbital rim, and 2 cm ventral to the line connecting the medial canthus to the infraorbital foramen. Trephining at this location provides access to the caudal maxillary sinus, and a view into the sphenopalatine sinus is possible.
-
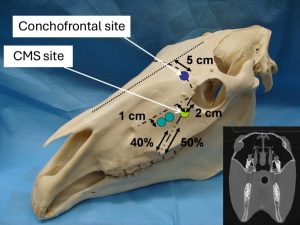
- Conchofrontal and maxillary sinus trephination sites.
Ruminant paranasal sinuses
Ruminants have a similar set of paranasal sinuses as the horse, with important anatomical differences and features.
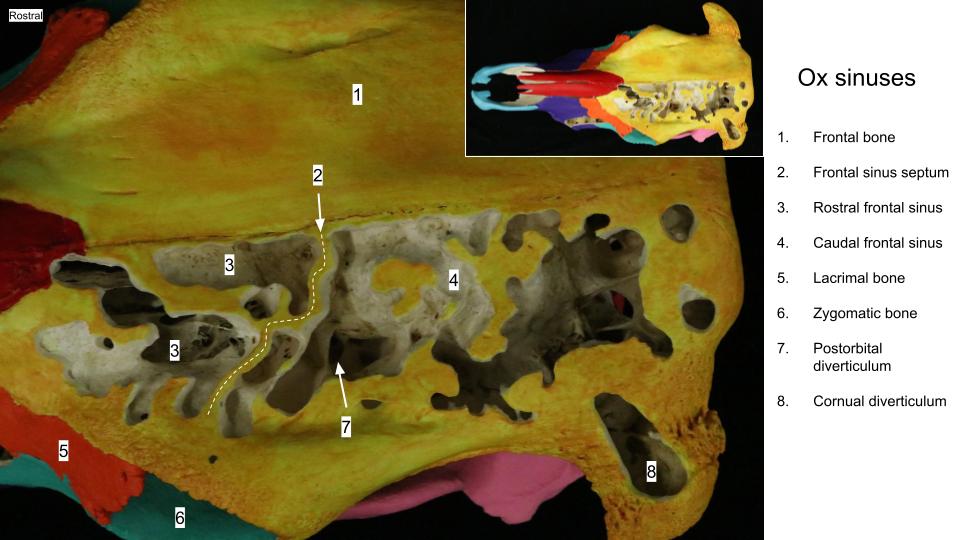
The frontal bones of the ox expand greatly as the calf matures into the adult, which accounts for the drastic change in head shape from the dome-like, “puppy skull” of the calf to the larger, more angular shape of the adult ox skull. This frontal expansion is related to the development of the large frontal sinuses, which continue to enlarge somewhat as the animal ages.
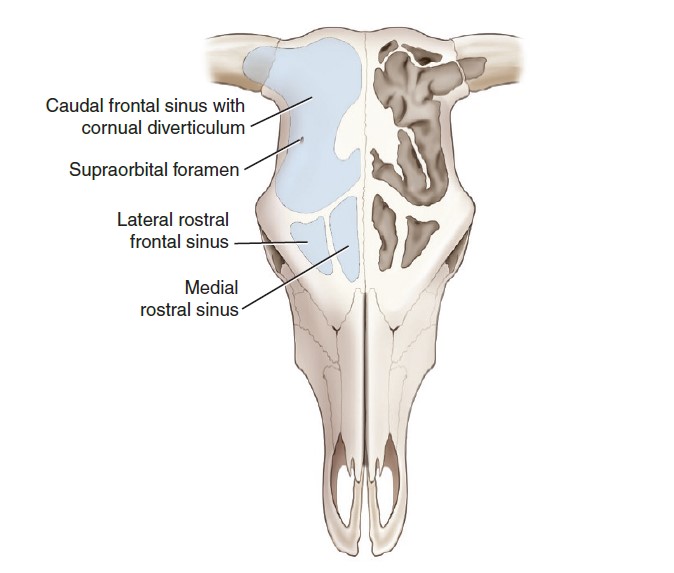
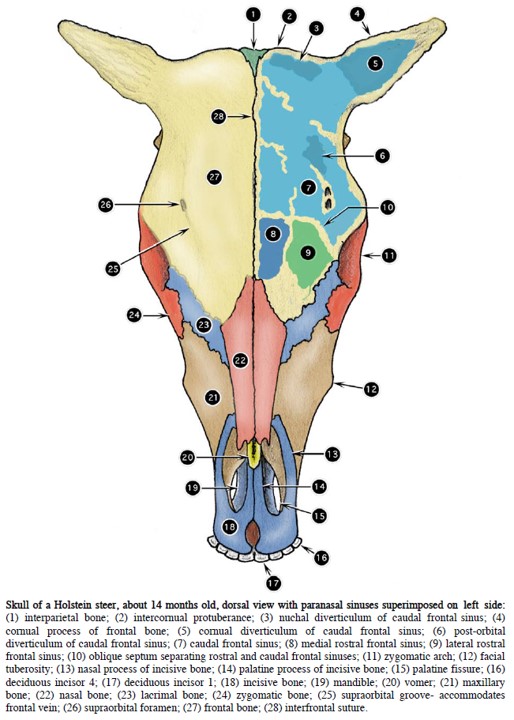
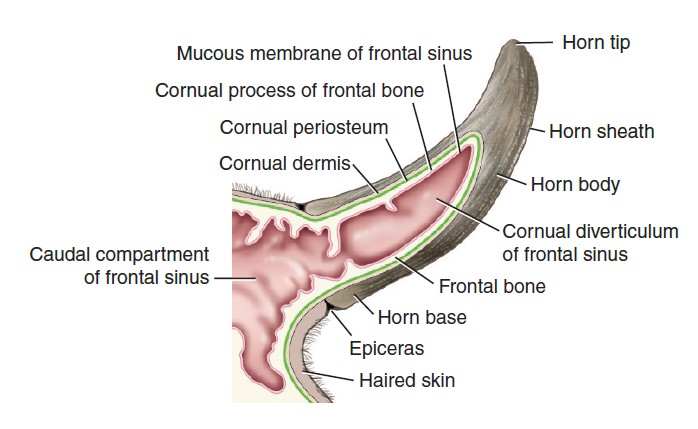
Unlike the horse, the frontal sinus of the ox is divided by an oblique frontal sinus septum into a large caudal frontal sinus and smaller rostral frontal sinus (which is further subdivided into medial and lateral compartments). The caudal frontal sinus contains a cornual diverticulum, which extends into the cornual process of the frontal bone, the process supporting the horn (see clinical relevance box). There is also a deep postorbital diverticulum and a nuchal diverticulum of the caudal frontal sinus. These recesses are difficult to adequately lavage and drain (see clinical relevance box). FYI – in small ruminants the frontal sinus is divided into a large lateral and smaller medial compartment only. In horned sheep and goats, it is the lateral frontal sinus that has the cornual diverticulum extending into the cornual process.
The various frontal sinuses of the ruminant drain separately into the nasal cavity, through openings at the ethmoidal conchae.
-
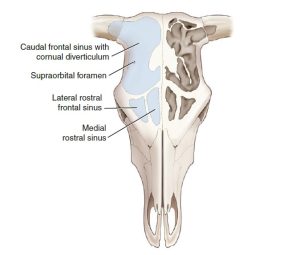
- Dorsal projection of the frontal sinuses of the ox. 9
-
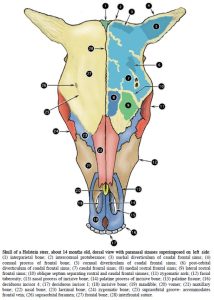
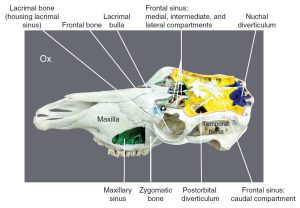
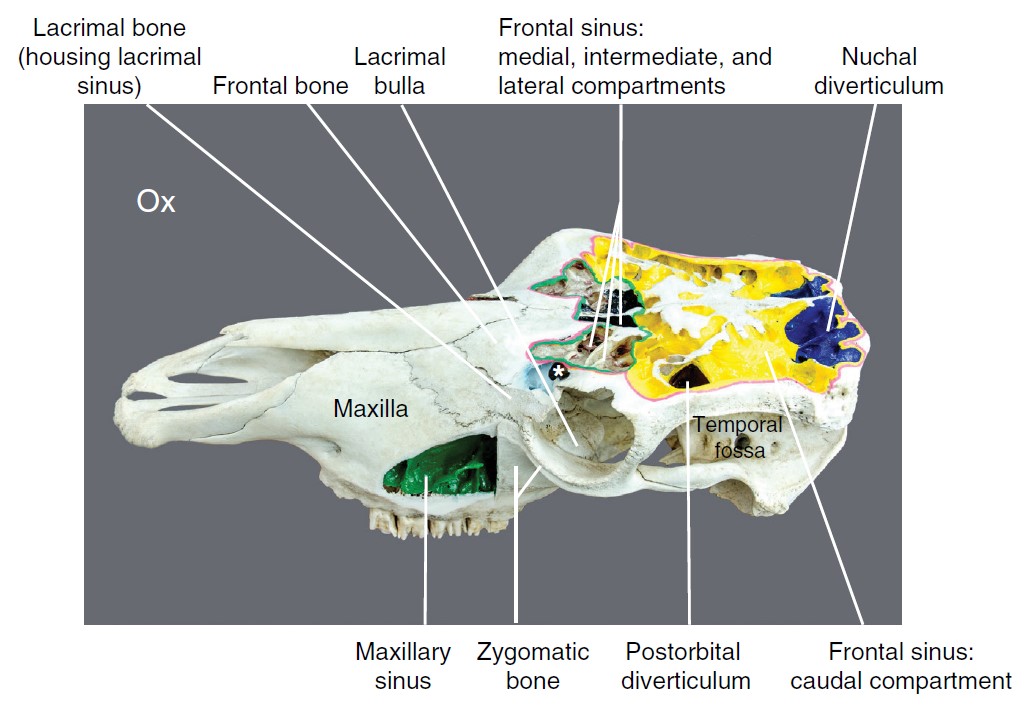
- Skull of a Holstein steer, about 14 months old, dorsal view with paranasal sinuses superimposed on left side. 2
-
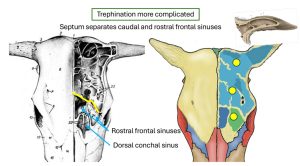
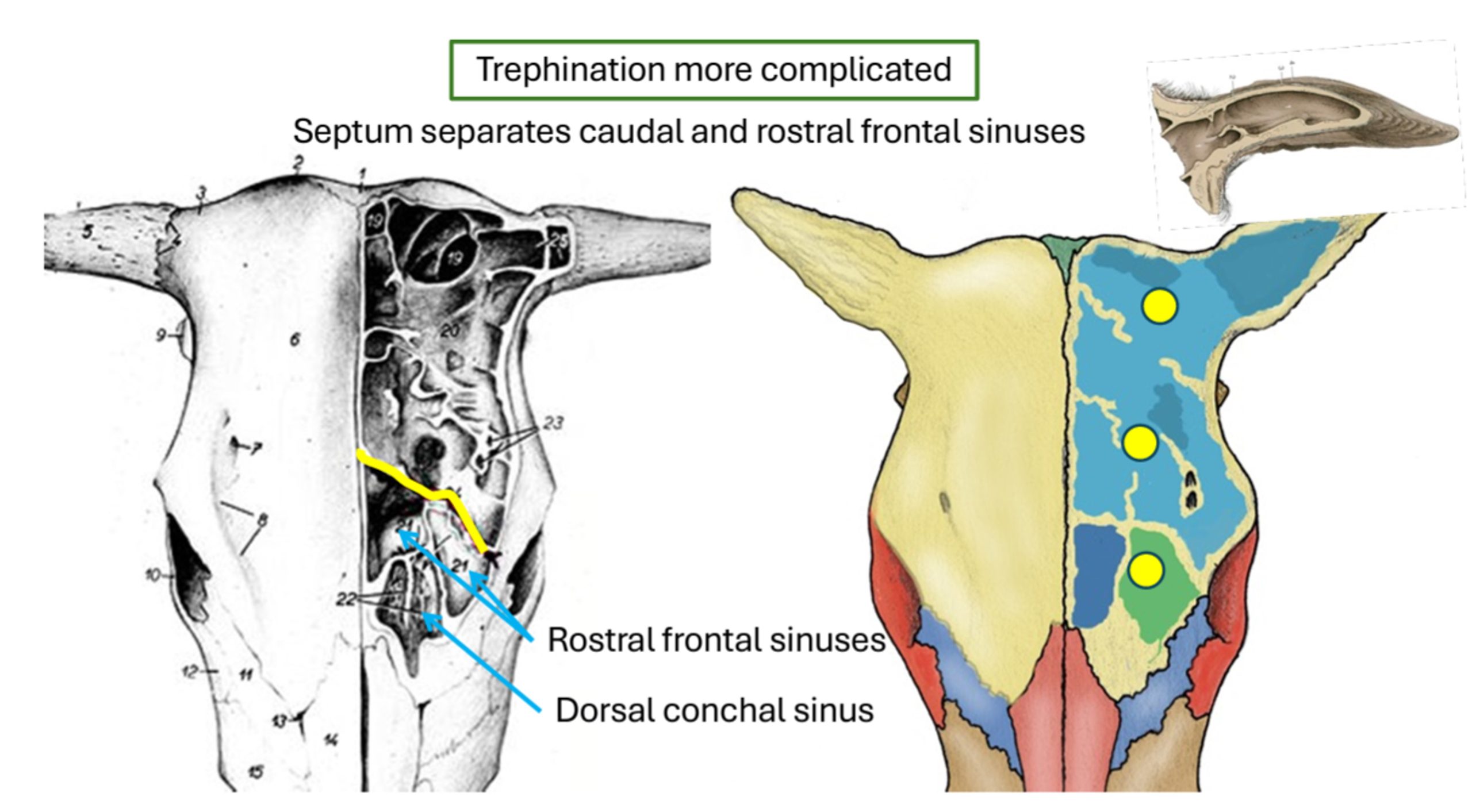
- Ox trephination.
Clinical relevance – frontal sinusitis, sinus access and sinus lavage
Infectious sinusitis is a potential sequela of dehorning when done after the cornual diverticulum has invaded the cornual process. Another scenario is when horns are “tipped” – shortened to remove the sharp points (for example in a rodeo bull) and the cornual diverticulum of the frontal sinus is inadvertently exposed. This leads to ascending infection of the sinus. The diverticula and the subdivisions of the ox frontal sinus complicate treatment of a sinus infection in this space. To access all the frontal sinuses for samples and treatment in the ox, multiple trephinations sites are necessary, to include at least one on either side of the frontal sinus septum.
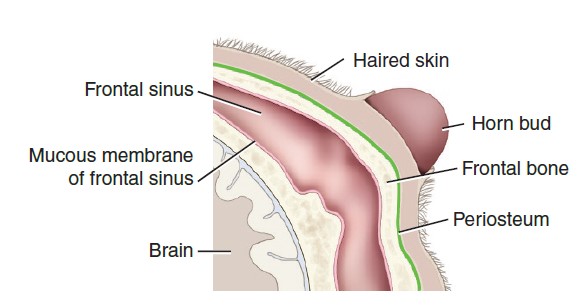
Avoiding opening the cornual diverticulum is one of many reasons it is preferred to disbud young ruminants before the horn bud attaches to the frontal bone instead of dehorning an adult animal.
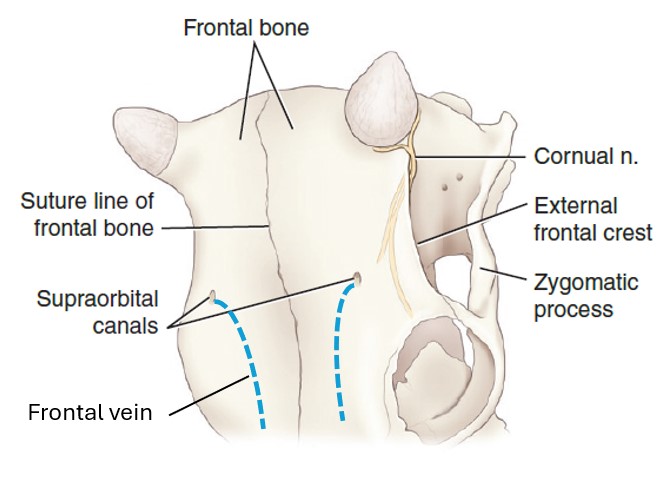
The supraorbital foramen is large and located medial to the orbit in the ox. The sizeable frontal vein emerges from the foramen and courses rostrally in a groove. This large vein should be avoided when trephination of the frontal sinus is performed.
-
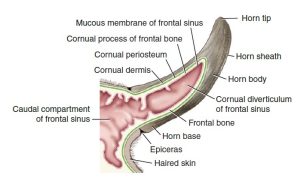
- Developed bovine horn. 9
-
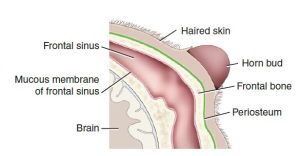
- Unattached horn bud. Before 2 months of age (in the calf), the horn bud is “floating” within the skin and not attached to the underlying frontal bone. 9
-
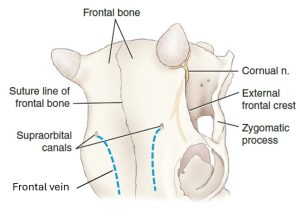
- Frontal vein of the ox. 9
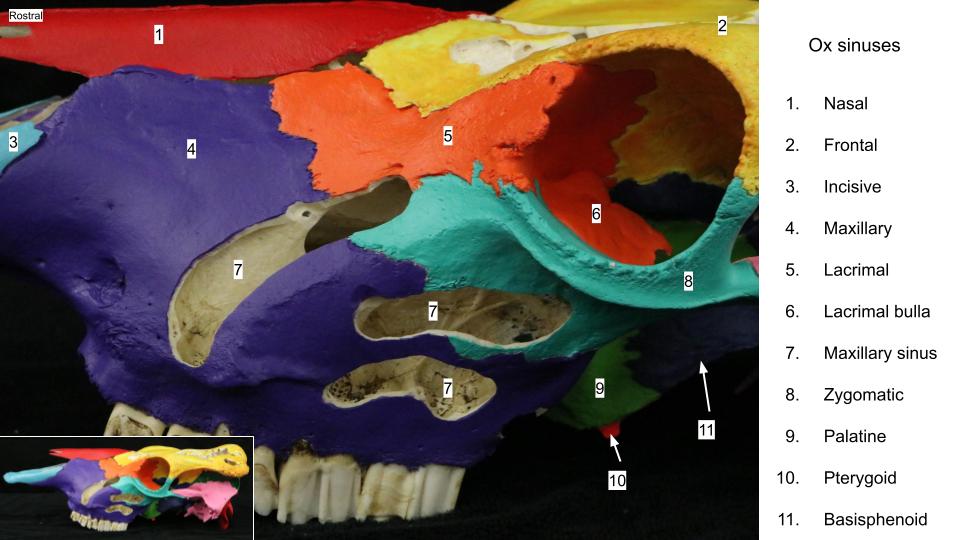
Also of important difference between the horse and ruminant, the maxillary sinus of the ox is not divided into rostral and caudal compartments, rather, it is a large singular space. The ruminant maxillary sinus has a clinically important diverticulum that extends caudally under the eye. This is the lacrimal bulla, which is an extremely thin-walled (eggshell) extension of the maxillary sinus (see clinical relevance box). The maxillary sinus drains into the nasal cavity at the middle nasal meatus. It also communicates with the lacrimal sinus and the palatine sinus.
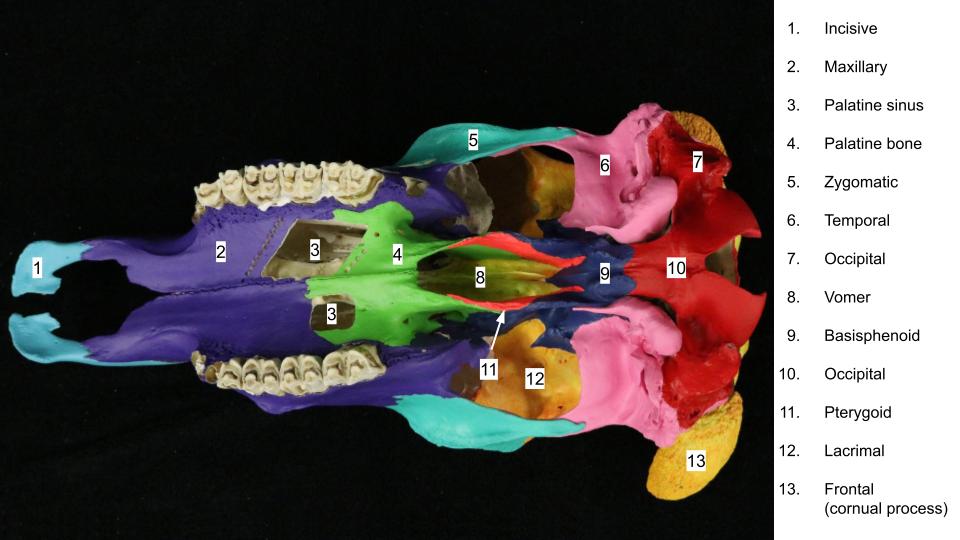
The sphenoid and palatine sinuses are independent in the ruminant. The palatine sinus is identified as an excavation of the hard palate and it communicates with the maxillary sinus over the dorsal aspect of the osseous infraorbital canal. The palatine sinus can be seen on the medial surface of the sectioned ruminant heads.
The lacrimal bone of the ruminant encloses a lacrimal sinus. This sinus should not be confused with the lacrimal bulla of the maxillary sinus. Conchal sinuses are also present in the ruminant, as in the horse.
-
- The lacrimal bulla is a very thin and excavated bony structure. It represents the caudal extent of the maxillary sinus. <sup12
-
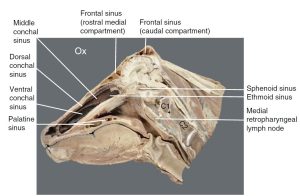
- Bovine head: sagittal section, showing the palatine sinus. 12
Clinical relevance – lacrimal bulla and exenteration
Because of its location, the lacrimal bulla is vulnerable to damage during orbital exenteration in the bovid. An exenteration (surgical removal of the eyeball and surrounding orbital tissues i.e. muscles, fat, nerves, periorbita) is usually carried out because of an advanced malignancy, typically squamous cell carcinoma or “cancer eye” in cattle.
Porcine paranasal sinuses – FYI
Although poorly developed or absent in the newborn pig, the extensive paranasal sinuses of the adult form a complex of air-filled spaces that almost completely surrounds the cranial cavity! The frontal sinuses are divided into rostral and caudal parts, and a large sphenoid sinus develops. The maxillary sinuses even invade the rostral parts of the zygomatic arches. Out of curiosity, refer to a skull specimen and note the extent of, and the many complicated diverticula in, the paranasal sinuses of the adult pig.
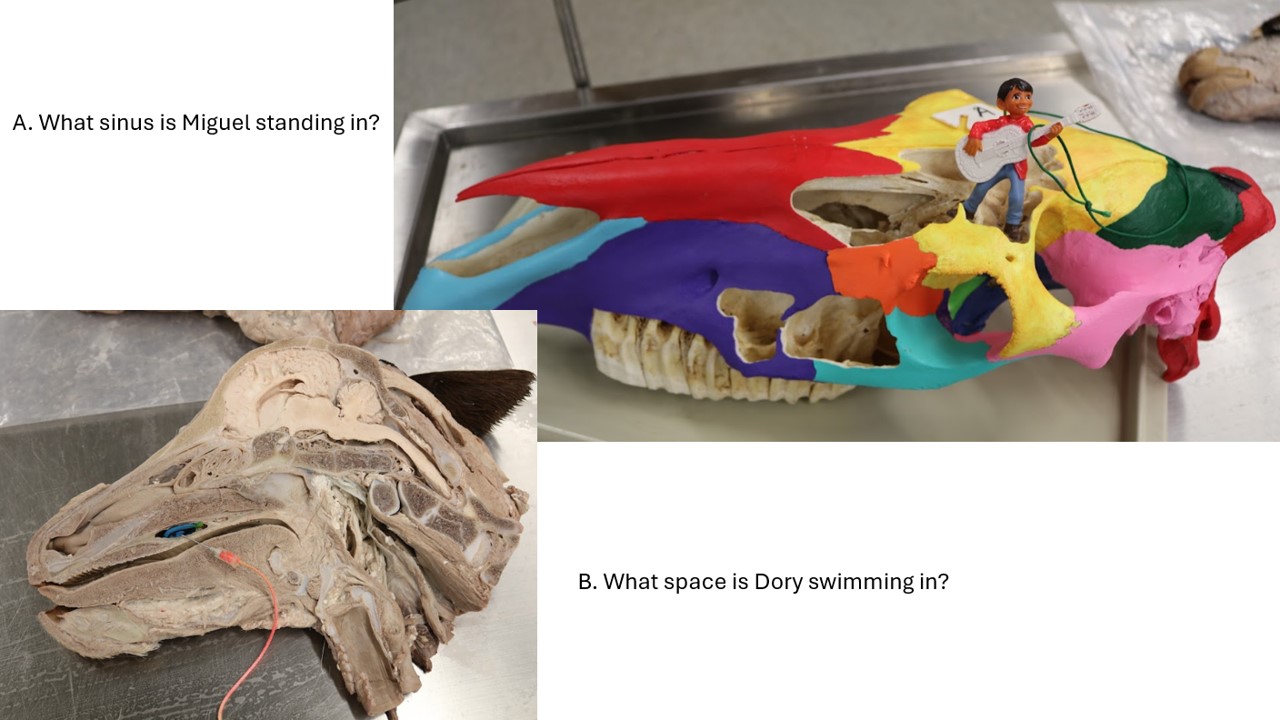
Clinical case question
 This horse is having sinoscopy performed, with the endoscope passed through a hole made into the paranasal sinuses. Based on the location of the entry point, which paranasal sinus is the endoscope entering (review figures of paranasal sinus anatomy).
This horse is having sinoscopy performed, with the endoscope passed through a hole made into the paranasal sinuses. Based on the location of the entry point, which paranasal sinus is the endoscope entering (review figures of paranasal sinus anatomy).
A – frontal sinus; B – rostral maxillary sinus; C – caudal maxillary sinus; D – dorsal conchal sinus; E – sphenopalatine sinus.
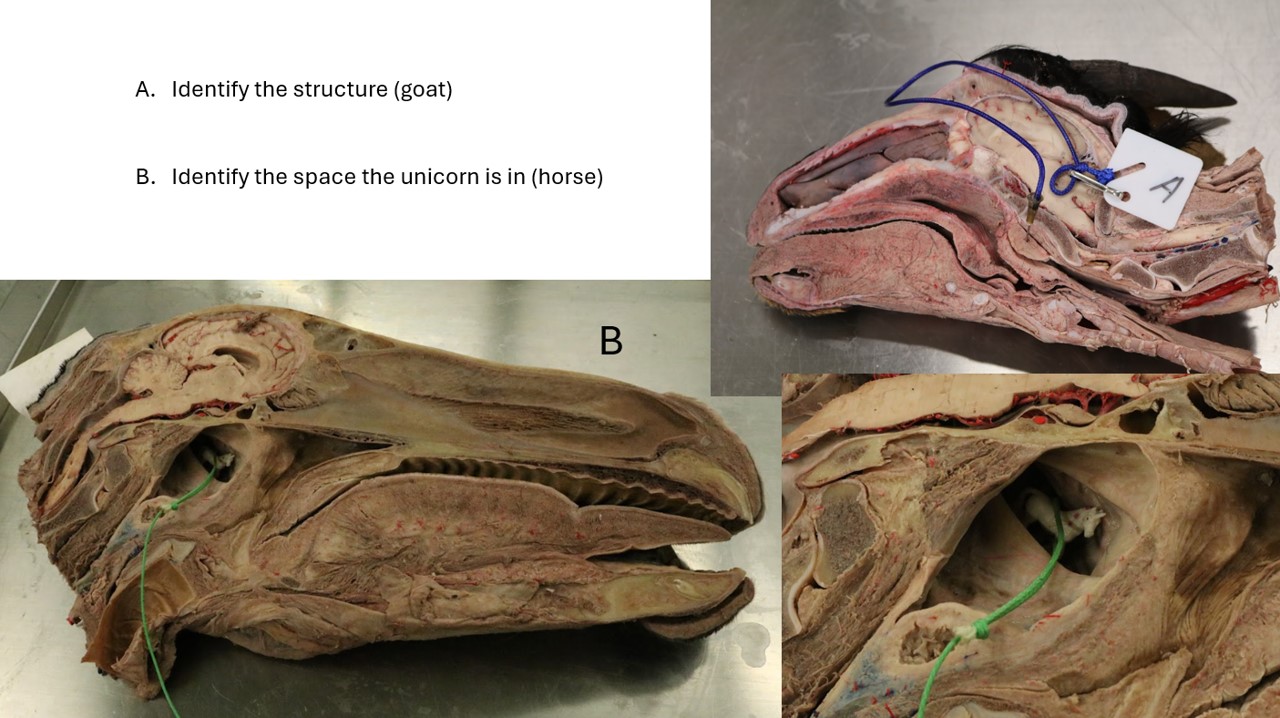
Guttural pouches and related structures – horse
(Guttur [L] = throat. Guttural means ‘of the throat’. ‘Guttural’ is used to describe a hoarse, harsh speech sound generated in the back of the throat. Please note that the correct spelling is guttural, not gutteral).
Observe: Retrieve prosected equine heads and examine the anatomy of the guttural pouches. Most structures are appreciated from the medial side that has had a deep dissection of the pouch and associated structures (nerves, vessels, lymph nodes, hyoid). Invariably the median septum is disrupted or removed to do the dissection. And the longus capitis and rectus capitis ventralis mm. may also have been excised. Most of the anatomy being reviewed has been previously studied (Nervous and Cardiovascular systems) and now it is time to put these structures in the context of the guttural pouch.
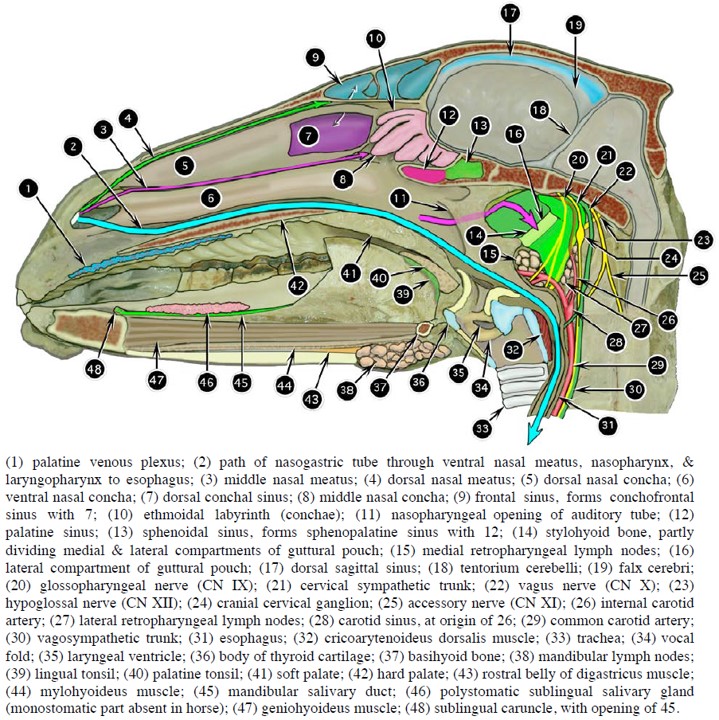
The guttural pouch is a diverticulum of the auditory (Eustacian) tube. The auditory tube passes from the tympanic cavity of the middle ear to the nasopharynx and allows for atmospheric pressure equalization across the tympanic membrane (eardrum). Guttural pouches are present in several wild species of perissodactyls (e.g., zebra, tapir), and are unique, among our domestic species, to equidae. There are left and right guttural pouches and their walls are comprised of a transparent, glistening respiratory mucosa. Each pouch normally contains about 300-500 ml of air. They are related dorsally to the base of the skull, atlas, axis, and several muscles, the largest of which is the longus capitis m. They lie dorsal and dorsolateral to the pharynx and larynx. Laterally the pouches are related to the deep surface of the parotid salivary glands. Vital cranial nerves and vessels pass in close association to the guttural pouches and the hyoid apparatus and retropharyngeal lymphocenters are also related.
-
- Guttural pouch casts. 10
-
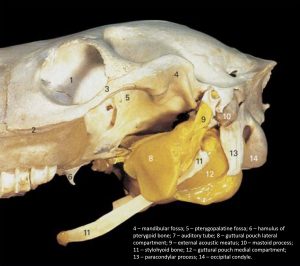
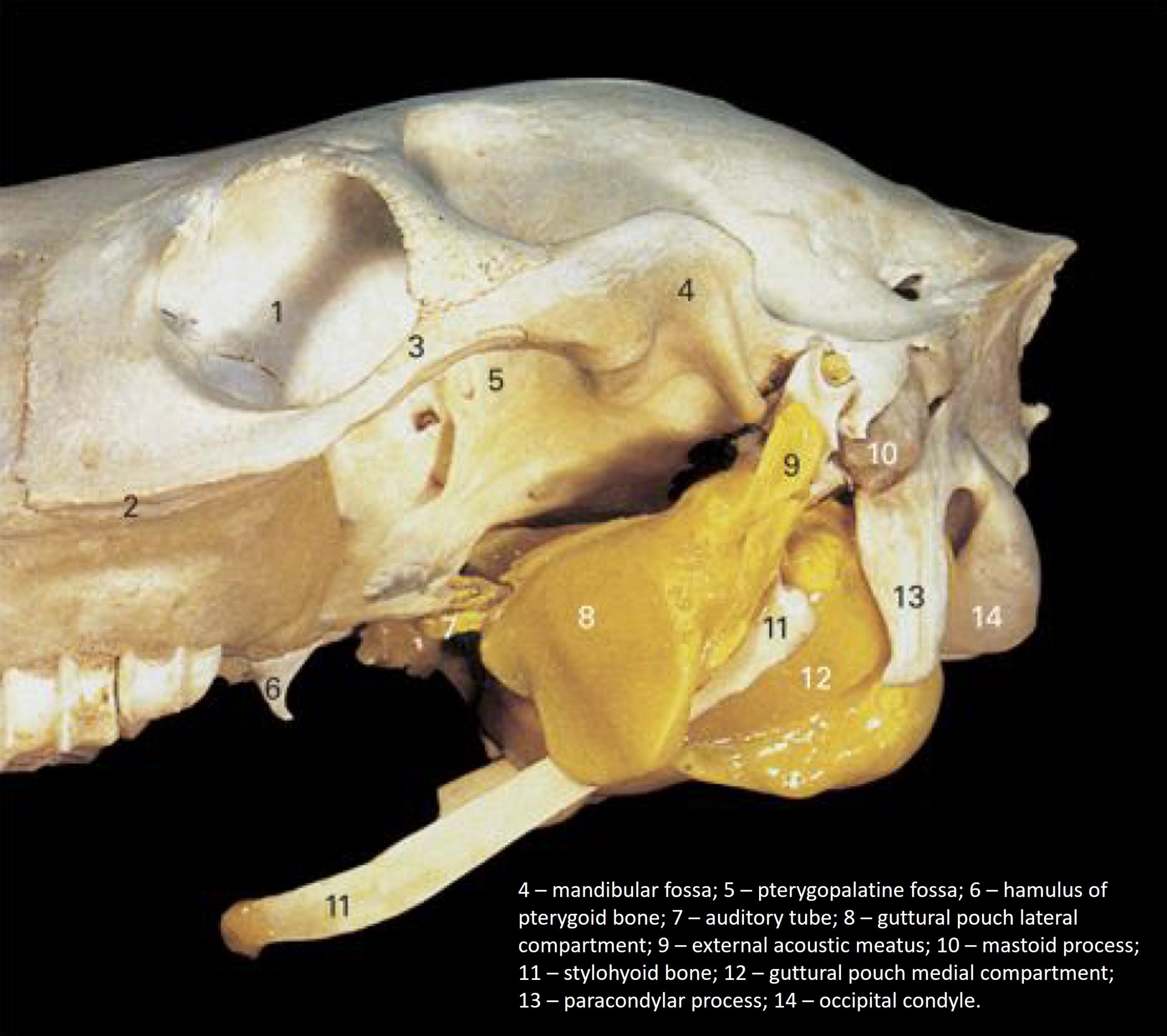
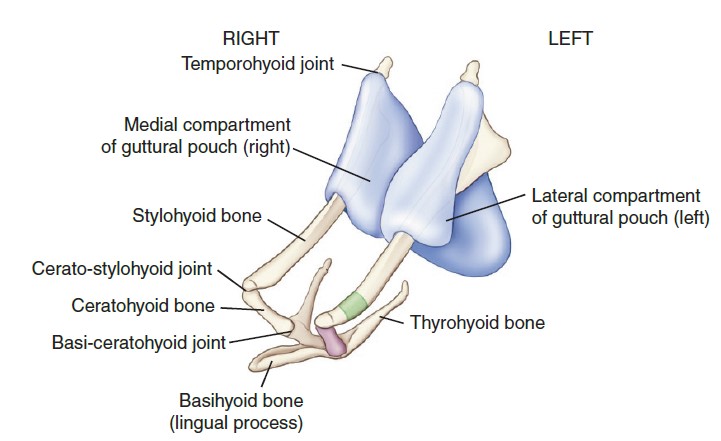
- Equine hyoid apparatus and its relation to the guttural pouches. 9
Clinical relevance – guttural pouch distention
Enlargement (distention) of one or both pouches can compress the pharynx and result in dyspnea and/or dysphagia. Distension may be due to excessive air in the pouch and this is called guttural pouch tympany.
-

- Guttural pouch tympany. 33

-

- Guttural pouch tympany. 8

Left and right guttural pouches are separated on midline by a median septum, the thin membrane where their medial walls are adjacent to each other. Caudodorsally the median septum is expanded and filled by the presence of the ventral muscles of the head—the longus capitis and rectus capitis ventralis muscles—as they insert on the basioccipital bone.
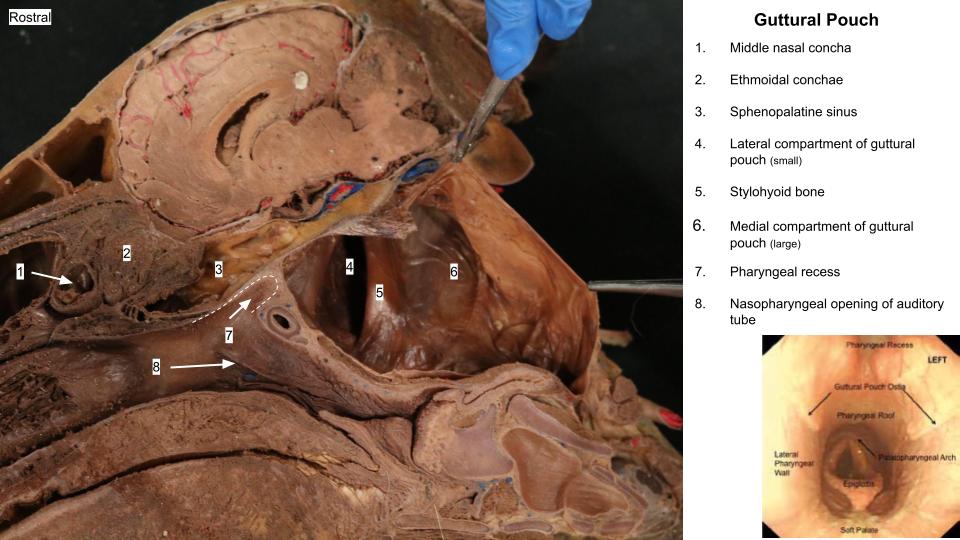
Each pouch is subdivided into a larger medial and smaller lateral compartment by the prominent stylohyoid bone, which indents the pouch ventrally. The attachment of the stylohyoid bone to the skull, forming the temporohyoid joint (THJ), is visible endoscopically, dorsocaudally in the pouch. The pouches are very closely related dorsomedially to the atlanto-occipital joint. Each pouch communicates with the nasopharynx by its ipsilateral pharyngeal opening of the auditory tube. The pharyngeal opening is funnel-shaped and the medial lamina of the opening is composed of fibrocartilage. The pharyngeal openings dilate during swallowing and are otherwise normally passively closed.
-
- Equine hyoid apparatus and its relation to the guttural pouches. 9
-
- Horse guttural pouch
Clinical relevance – temporohyoid osteoarthropathy
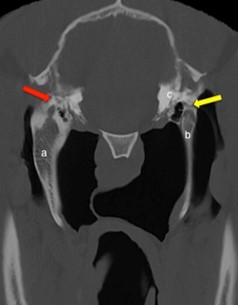
Clinical relevance: Disease of the temporohyoid joint and adjacent stylohyoid bone is called temporohyoid osteoarthropathy (THO). This condition is associated with clinical signs of cranial nerve VII and VIII dysfunction. Pouch endoscopy and CT examination are the diagnostic imaging of choice; radiographs can also be diagnostic but are less sensitive. Medical and surgical therapies are described.
-

- Characteristic signs of a horse with left sided temporohyoid osteoarthropathy resulting in an ear and lip droop due to dysfunction of cranial nerve 7. 34
-
- Endoscopic image of the guttural pouch with enlarged stylohyoid bone (white arrow). 34
-
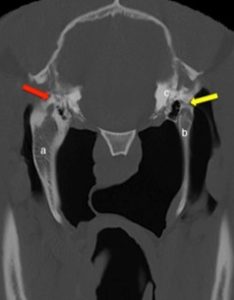
- CT Scan of a horses’ temporohyoid joints. One sided is affected by temporohyoid osteoarthroapthy (red arrow) and the other side is normal (yellow arrow). 34
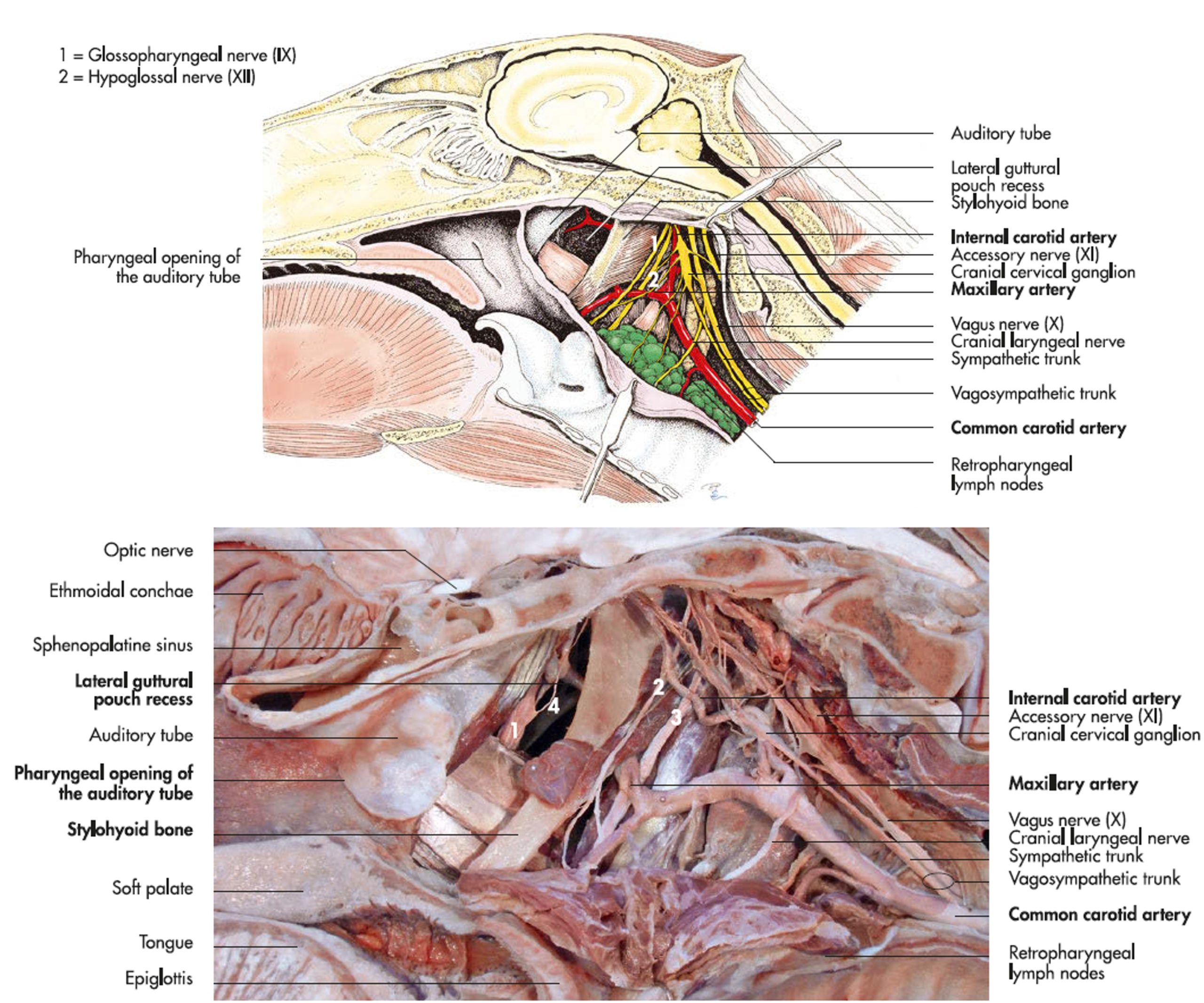
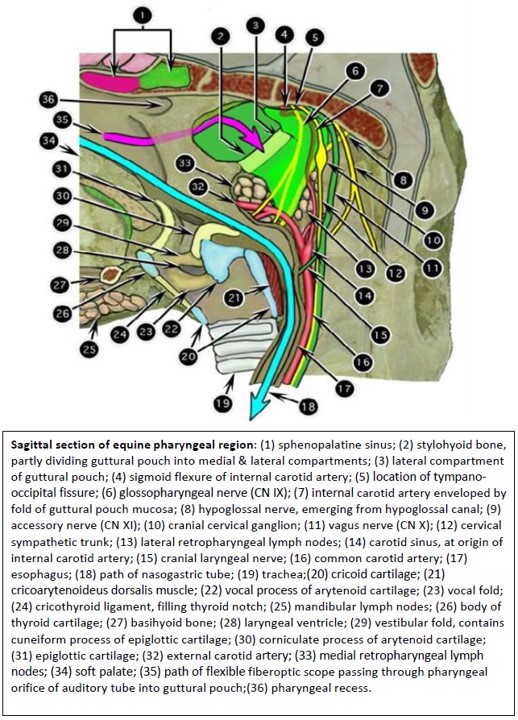
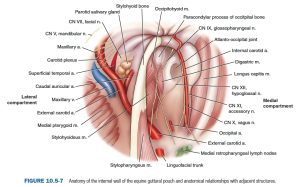
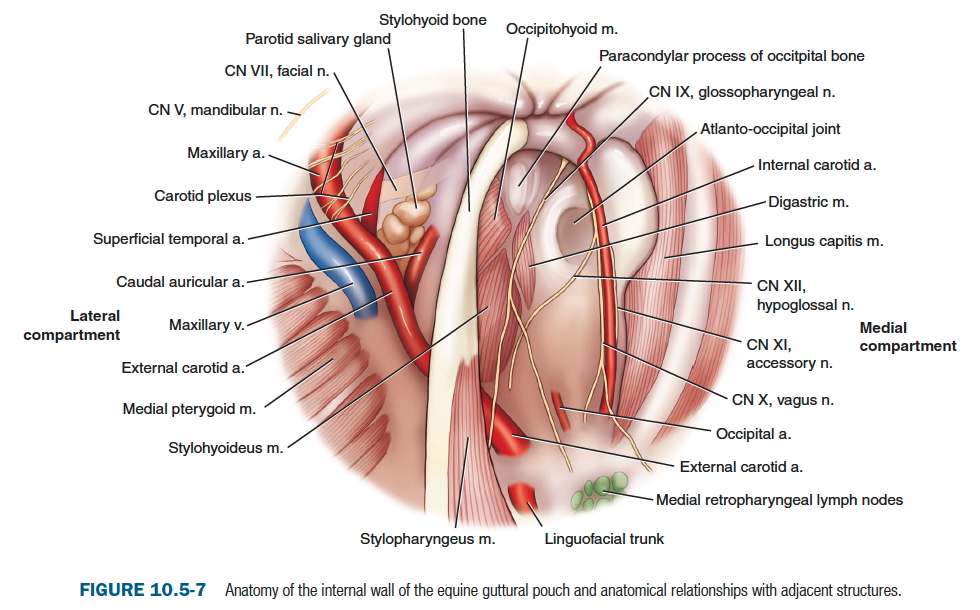
Multiple vessels and nerves track directly behind the transparent mucosal walls of both guttural pouch compartments (recall, these structures were studied in the Nervous and Cardiovascular systems). These vessels and nerves are visible during endoscopic examination and are vulnerable to guttural pouch disease. The internal carotid artery and cranial nerves IX, X, XI, and XII pass in the caudal wall of the medial compartment. The sympathetic trunk and its cranial cervical ganglion are also in the vicinity. Ventrally, the external carotid artery is associated with the floor of the medial compartment before it passes deep to the stylohyoid bone and is then associated with the wall of the lateral compartment. In the lateral compartment, the external carotid artery provides the caudal auricular artery close to the stylohyoid bone, and then continues as the maxillary artery in the dorsal wall of the lateral compartment, after the superficial temporal artery branches off. The maxillary vein lies adjacent to the external carotid artery in the lateral compartment. Cranial nerves VII and VIII pass in close proximity to the temporohyoid joint, and may be affected by disease of the joint (see clinical relevance box). CN VII is also related to the dorsocaudal wall of the lateral compartment.
-
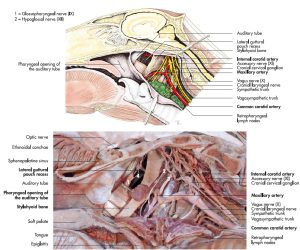
- Topography of the right guttural pouch of the horse. 7
-

- Sagittal section of equine pharyngeal region. 2
-
- Guttural pouch wall anatomy as viewed endoscopically.9
Clinical relevance – clinical signs of GP disease related to CNs
Disease of the guttural pouch may cause dysfunction of any of the nervous structures in the region. Signs of facial n. paralysis (CN VII) and vestibular disease (CN VIII) have been mentioned with THO. Dysphagia can result from CN IX and X dysfunction. Laryngeal hemiplegia can result from CN X dysfunction. Successful treatment of the disease does not always lead to resolution of the clinical signs of nerve dysfunction, leading to long term complications.
Clinical relevance – GP disease and hemorrhage
Guttural pouch mycosis is caused by opportunistic fungus (Aspergillus fumigatus) and can have serious consequences. The growing fungus can erode the thin respiratory mucosal wall of the pouch and then the wall of an artery, causing life-threatening hemorrhage. The internal carotid a. is commonly affected, however the other large arteries are at risk. Acute, severe epistaxis accompanies artery rupture and it may be the first clinical sign noted, of a fungal infection. Horses that survive a bleed or are diagnosed before hemorrhage occurs are managed by efforts to eliminate the fungus and protect against a terminal hemorrhage event. Fungal infections can erode into the nasopharynx or through the median septum, creating permanent openings.
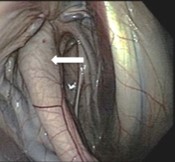
Below is an endoscopic view of a horse’s nasopharynx, looking caudally towards the larynx. This horse has a history of sudden onset profuse nasal hemorrhage (epistaxis), that slowed after a few minutes, and the horse was referred on emergency for work up. From what opening is the blood exiting?
A – the laryngopharynx and start of the esophagus
B – the entrance to the larynx
C – the pharyngeal opening of the auditory tube
D – the nasomaxillary opening.

Both medial and lateral retropharyngeal lymph nodes are associated with the wall of the guttural pouch, and the two groups often coalesce at the division of the common carotid artery. The larger medial retropharyngeal lymph nodes are those most closely associated with the wall of the pharynx, lying under the floor of the medial compartment. The lateral nodes lie more on the caudodorsal aspect of the pouch near the internal carotid artery and wing of the atlas. Because of the close relationship of these two groups of nodes in the horse, they can be considered collectively as retropharyngeal lymph nodes (these lymph nodes were also studied in the Cardiovascular unit).
-
- Topography of the right guttural pouch of the horse. 7
-
- Sagittal section of equine pharyngeal region. 2
-
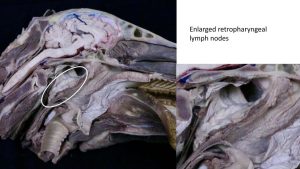
- Retropharyngeal lymph nodes
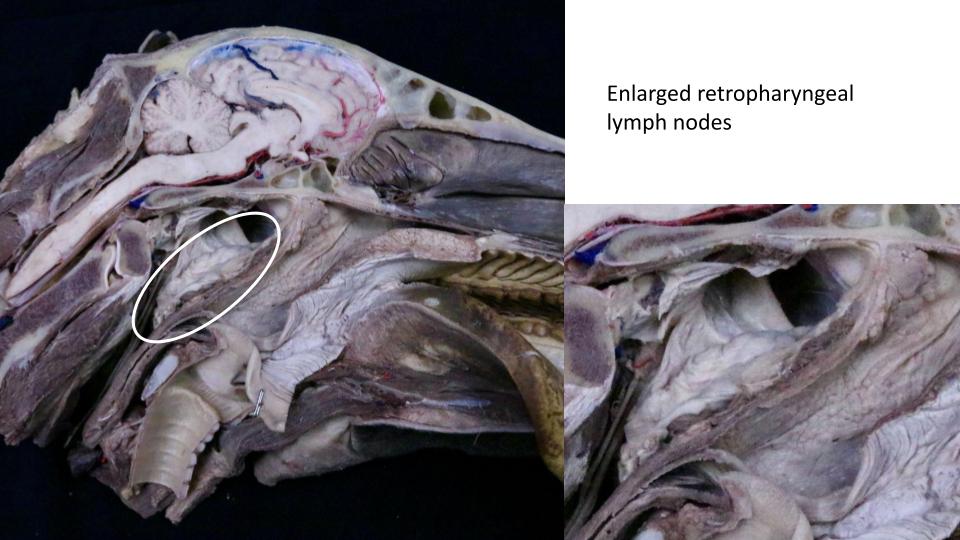
Clinical relevance – “Strangles”
The guttural pouches frequently become involved in upper respiratory infections. Guttural pouch empyema refers to a pouch filled with pus, often secondary to Streptococcus equi subsp. equi infection. One pathway of infection is via the retropharyngeal lymph nodes – they abscess and rupture into the guttural pouch. Swollen, infected lymph nodes put pressure on the pharynx and larynx causing dyspnea and dysphagia – the clinical disease is known as “Strangles”. Lavage and drainage of the guttural pouch may be necessary for treatment. Recall Viborg’s triangle – a surgical approach to the guttural pouch, not used much anymore due to risk of damage to neurovascular anatomy around the pouch. There are better approaches.
-

-
Streptococcus equi infection. This Welsh Mountain Pony has a resolving retropharyngeal
lymph node abscess. This photograph was taken approximately 4 weeks after the onset of clinical signs. 33

-
-
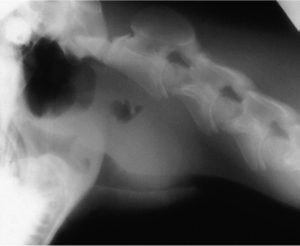
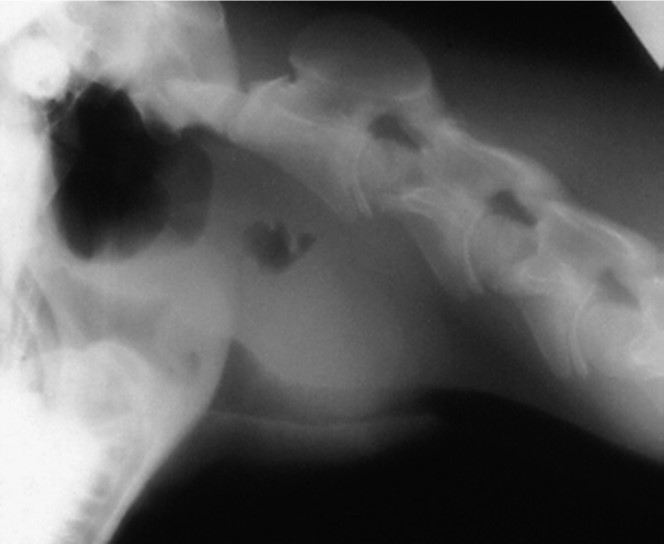
Streptococcus equi infection. Large, non-ruptured retropharyngeal
lymph nodes may compress the nasopharynx and trachea causing dyspnea. This radiograph shows ventral deviation of the trachea by a large retropharyngeal lymph node abscess. 33
FYI – What’s the Purpose of the Guttural Pouches Anyway? Dr. Smallwood suggests the following (paraphrased): “The guttural pouches have little, if anything, to do with the respiratory system, and serve primarily a cardiovascular function. In addition to cooling the arterial blood prior to reaching the brain, the pouches may also function to regulate intracranial blood pressure through their intimate relationship with the internal carotid artery. My hypothesis is that the guttural pouches of the horse serve as “pneumatic cuffs” around the internal carotid arteries, and work in the following way. When a horse lowers its head to graze or drink, the abundant soft tissues on the caudodorsal aspect of the pouch (lymph nodes, salivary tissue, etc.) fall forward and compress the pouch. Assuming the horse can concurrently close off the pharyngeal opening, air pressure within the pouch goes up (like in a blood pressure cuff) and the artery, suspended in its little “mesartery” and surrounded by air, is compressed. This compression reduces the diameter of the artery, thereby increasing resistance and serving to prevent a high-pressure surge of blood pressure into the cerebral circulation until the baroreceptor reflex can accommodate for the change in hemostatic pressure. In essence, the horse has solved the same problem as the ruminant and cat with their rete mirabile, by using an entirely different strategy.
Review videos
Horse and ruminant paranasal sinuses – 8 min
Horse guttural pouch – 1 min, watch until 8 min
Cranial nerves associated with the guttural pouch – 6 min, watch until 11:30
Terms
| Paranasal sinuses | |
| Features | Comments, horse, ox, or both |
| Frontal sinus | horse and ox |
| Rostral frontal sinus | ox |
| Frontal sinus septum | ox, divides caudal and rostral parts |
| Caudal frontal sinus | ox |
| cornual diverticulum | ox |
| nuchal diverticulum | ox |
| post-orbital diverticulum | ox |
| Dorsal conchal sinus | horse |
| Ventral conchal sinus | horse |
| Middle conchal sinus | horse |
| Conchofrontal sinus | horse, combined space of frontal and dorsal conchal |
| Maxillary sinus | horse and ox |
| Lacrimal bulla | ox, maxillary sinus extension into space of orbit |
| Caudal maxillary sinus | horse |
| Maxillary sinus septum | horse, divides rostral and caudal parts |
| Rostral maxillary sinus | horse |
| Frontomaxillary opening | horse: conchofrontal to caudal maxillary sinus |
| Nasomaxillary (sinonasal) opening | horse: maxillary sinuses to nasal cavity, located at caudal end of middle nasal meatus |
| Infraorbital canal | horse, feature of maxillary sinus anatomy |
| Sphenopalatine sinus | horse |
| Palatine sinus | ox, located in hard palate |
| Guttural Pouches – Horse |
|
| Guttural pouch | left and right pouches are present |
| Lateral compartment | |
| Medial compartment | |
| Median septum | mucosal and muscle parts |
| Stylohyoid bone | |
| Pharyngeal opening of auditory tube | opening in nasopharynx, endoscopic access to GP |
| Internal carotid a. | |
| External carotid a. | |
| Retropharyngeal lnn. | medial and lateral – learn as one cluster |
| CNs X, XII | |
| CNs VII, VIII, IX, XI | not to identify, be aware of clinical signs of GP disease |
| Sympathetic trunk and cranial cervical ganglion | not to identify, be aware part of GP wall anatomy |
| Longus capitis m. | not to identify, be aware of clinical signs of GP disease |
| Rectus capitis ventralis m. | not to identify, be aware of clinical signs of GP disease |