Lab 5A: The Abdominal Cavity of the Carnivore (pt. 1)
Learning Objectives
- Define abdominal cavity and peritoneal cavity.
- Name and identify the parietal, visceral, and connecting peritonea of the abdomen.
- Apply the embryology of gut and peritoneum development to identify and understand the location and function of the abdominal viscera and peritoneum in the cat and dog.
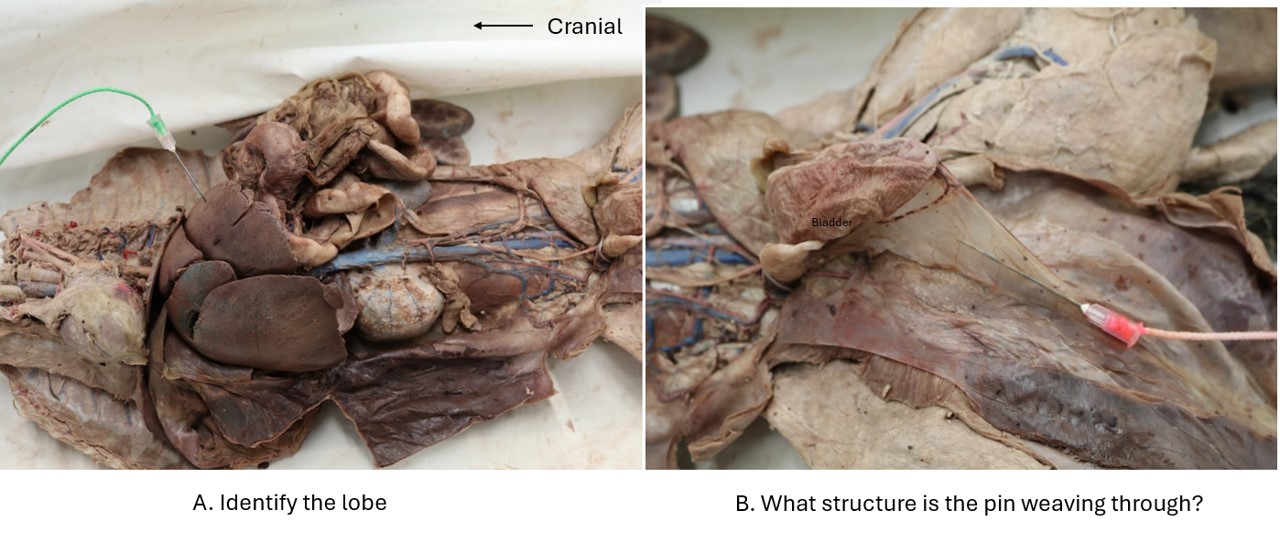
- Identify the lobes of the liver.
- Identify parts of the stomach.
Lab Instructions
Opening the Abdominal Cavity
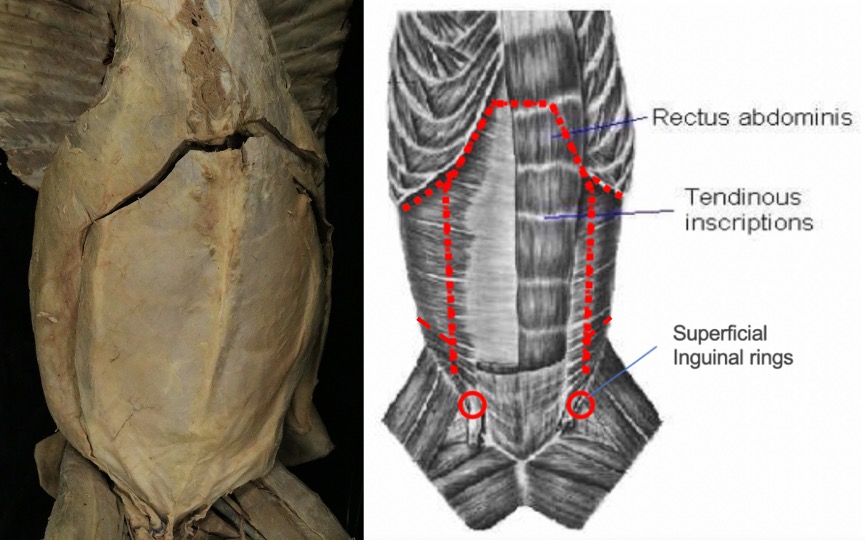
Dissect: As the following incisions are made, be careful of the depth of the incision to avoid incising any viscera in the abdominal cavity. Starting just caudal to the costal arch, make a full thickness longitudinal incision, parallel to and ~1cm dorsal to the beginning of the aponeurosis of insertion of the external abdominal oblique m. Perform this incision on both sides. Extend the incisions caudally until the level of the umbilicus.
Connect the left and right incisions cranially by incising along the costal arch and then transversally just caudal to the xyphoid process. Also incise along the caudal margin of the costal arch dorsally on both sides to further open the abdomen.
Continue the longitudinal incisions caudally from the umbilicus, stopping a few centimeters cranial to the inguinal canal anatomy. Lastly, as needed for improved caudal abdomen access, make incisions through the muscular wall heading dorsally, starting at the caudal end of the longitudinal incisions. Reflect the superficial fascia from the lateral abdominal wall.
The Abdominal Cavity
The abdominal cavity is formed by the muscles of the abdominal wall, the ribs, and the diaphragm. It is lined by peritoneum, which encloses the peritoneal cavity.
The peritoneal cavity, like the pleural and pericardial cavities, is a closed space. It is lined by a serous membrane, called the peritoneum. Serous membranes are thin layers of loose connective tissue covered by a layer of mesothelium. The peritoneum is derived from the somatic and splanchnic mesodermal layers lining the embryonic coelom.
The peritoneum can be divided into three regional components. The parietal peritoneum is the layer that lines the inner abdominal (and pelvic cavity) body wall and has to be incised to open the peritoneal cavity. The transversalis fascia, fascia lying immediately deep to the peritoneum, reinforces the parietal peritoneum and attaches it to the abdominal muscles and diaphragm. The visceral peritoneum covers (i.e. intimately surrounds) the organs suspended in these cavities. Therefore, there are no organs “within” the peritoneal cavity (recall, just the same as there are no organs “within” the pleura cavities) because they are all covered by visceral peritoneum. (Only an oocyte when it ovulates is briefly within the peritoneal cavity before it enters the uterine tube.) The connecting peritoneum is a double sheet of peritoneum that connects the parietal and visceral layers or the visceral layers of adjacent organs, forming peritoneal folds referred to as mesenteries, omenta, or ligaments.
In the embryo the dorsal common mesentery is a double layer of connecting peritoneum that passes from the dorsal abdominal wall to the digestive tube. It serves as a route by which the nerves and vessels reach the organs. In the embryo, the dorsal common mesentery persists from cranial to caudal as the greater omentum, mesoduodenum, mesentery, and mesocolon.
Peritoneums will be discussed throughout this unit, in relation to their association with abdominal viscera. We will consider a few related to the ventral body wall, liver and urinary bladder next.
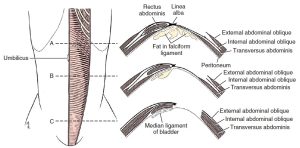
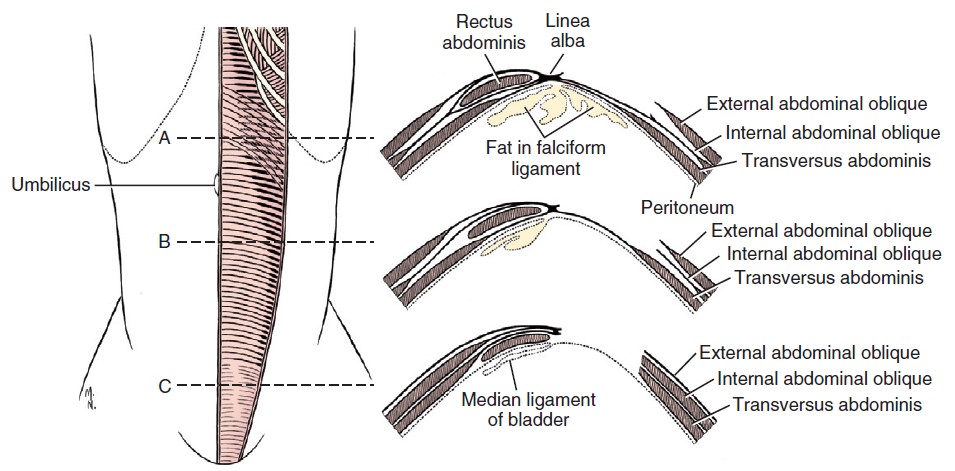
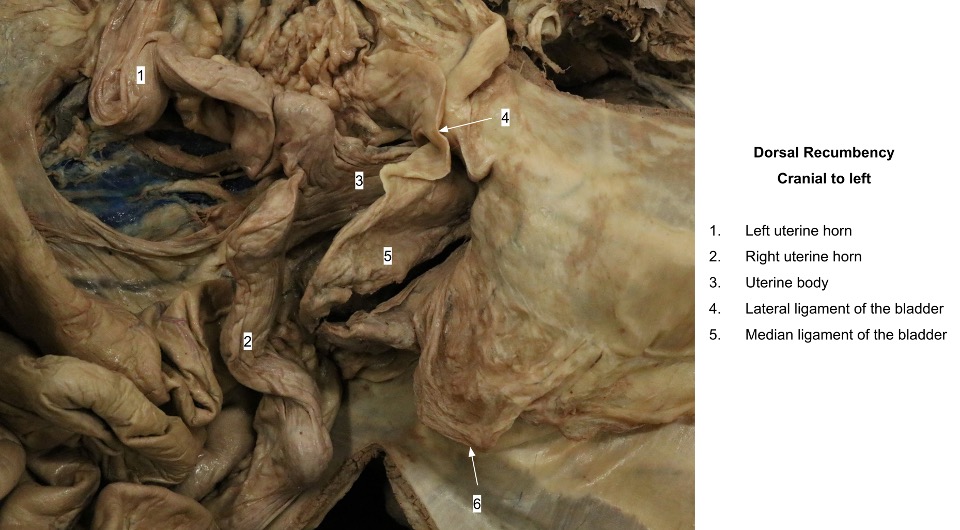
The falciform ligament is a fold of connecting peritoneum that passes from the umbilicus to the diaphragm. It is also attached to the liver between the left medial and quadrate lobes. In obese specimens a large accumulation of fat is found in this remnant of the embryonic ventral mesentery. In young animals the round ligament of the liver may still be visible in the free border of the falciform ligament. In the fetus the umbilical vein courses cranially in the free border of the falciform ligament to enter the liver, and this umbilical vein atrophies and fibrosis after birth to form the round ligament of the liver. Caudal to the umbilicus, the fold of connecting peritoneum is the median ligament of the bladder. In the fetus, the urachus and umbilical arteries pass along the free border of the median ligament of the bladder.
-
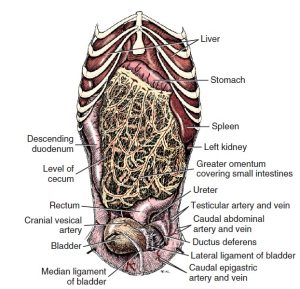
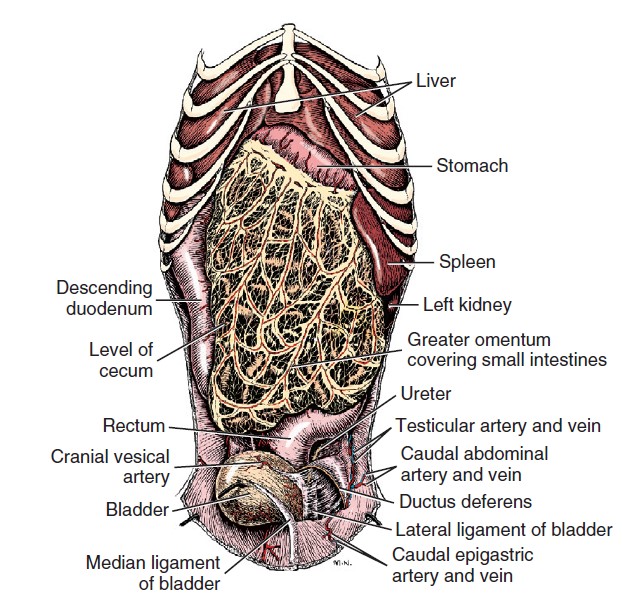
- Abdominal viscera of male dog, ventral aspect. 1
-
- Falciform ligament. 1
-

- Greater omentum
-

- Ligaments of the bladder
-

- Falciform ligament
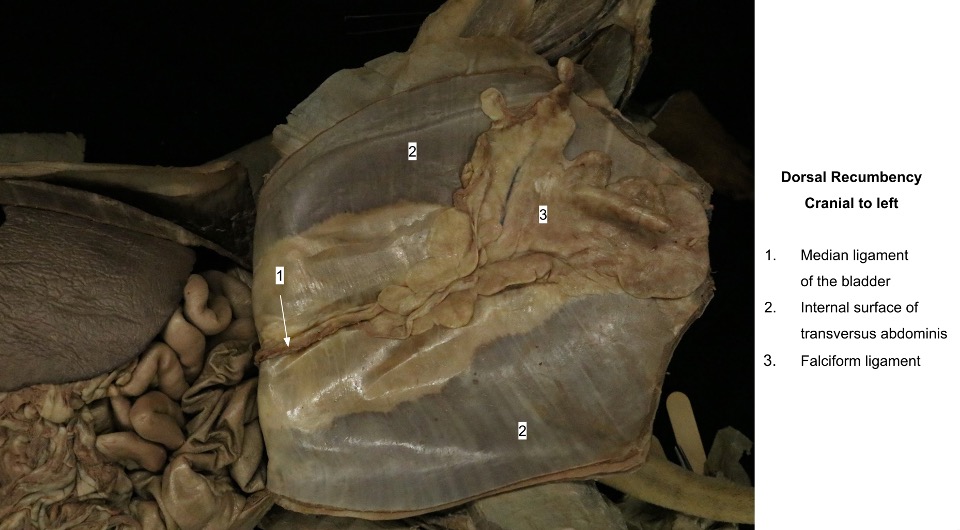
Observe: Observe the falciform ligament, its free border – the round ligament of the liver, and the median ligament of the bladder in the opened abdominal cavity.
The Greater and Lesser Omentum
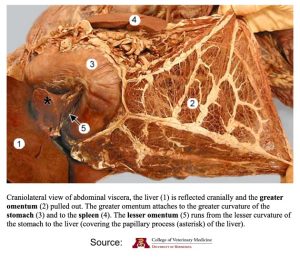
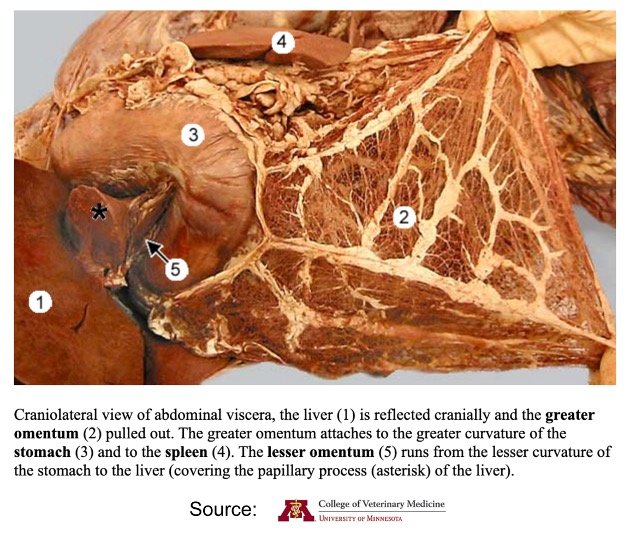
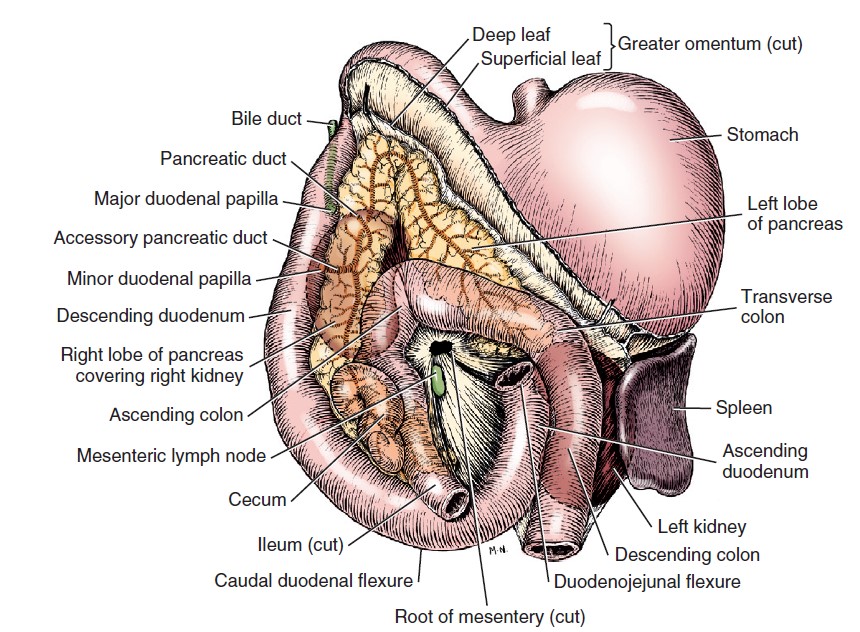
An omentum (pl. omenta) is the connecting peritoneum that attaches the stomach to the dorsal body wall or other organs. The greater omentum is the first structure seen after reflecting the abdominal wall. It is a caudoventral extension of the two layers of connecting peritoneum that pass from the dorsal body wall to the greater curvature of the stomach, the dorsal mesogastrium. The greater curvature of the stomach is along the caudal margin of the stomach. The greater omentum is lacelike, with depositions of fat along the vessels. It covers the jejunum and ileum, leaving the descending colon exposed on the left, the bladder exposed caudally, and the descending duodenum exposed on the right.
Observe: Observe the greater omentum in your cadaver covering the structures listed above. Note that in some animals, a substantial amount of fat may have accumulated within the greater omentum.
The greater omentum has two distinct layers, the superficial and deep leaves. The space between these layers is called the omental bursa. As the stomach formed and rotated to its definitive position in the embryo, this mesogastrium grew extensively and formed a double-layered sac that extends caudoventrally beneath many of the abdominal organs. From the greater curvature of the stomach, it extends caudally within the peritoneal cavity as the superficial leaf between the jejunum and the ventral abdominal wall (the superficial leaf is seen first after entering the peritoneal cavity through a ventral midline incision). The spleen is enveloped by an outpocketing of the superficial leaf. The superficial leaf turns dorsally on itself near the pelvic inlet and returns as the deep leaf dorsal to the stomach, where it contains the left lobe of the pancreas between its peritoneal layers.
-
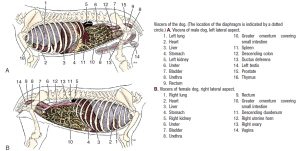
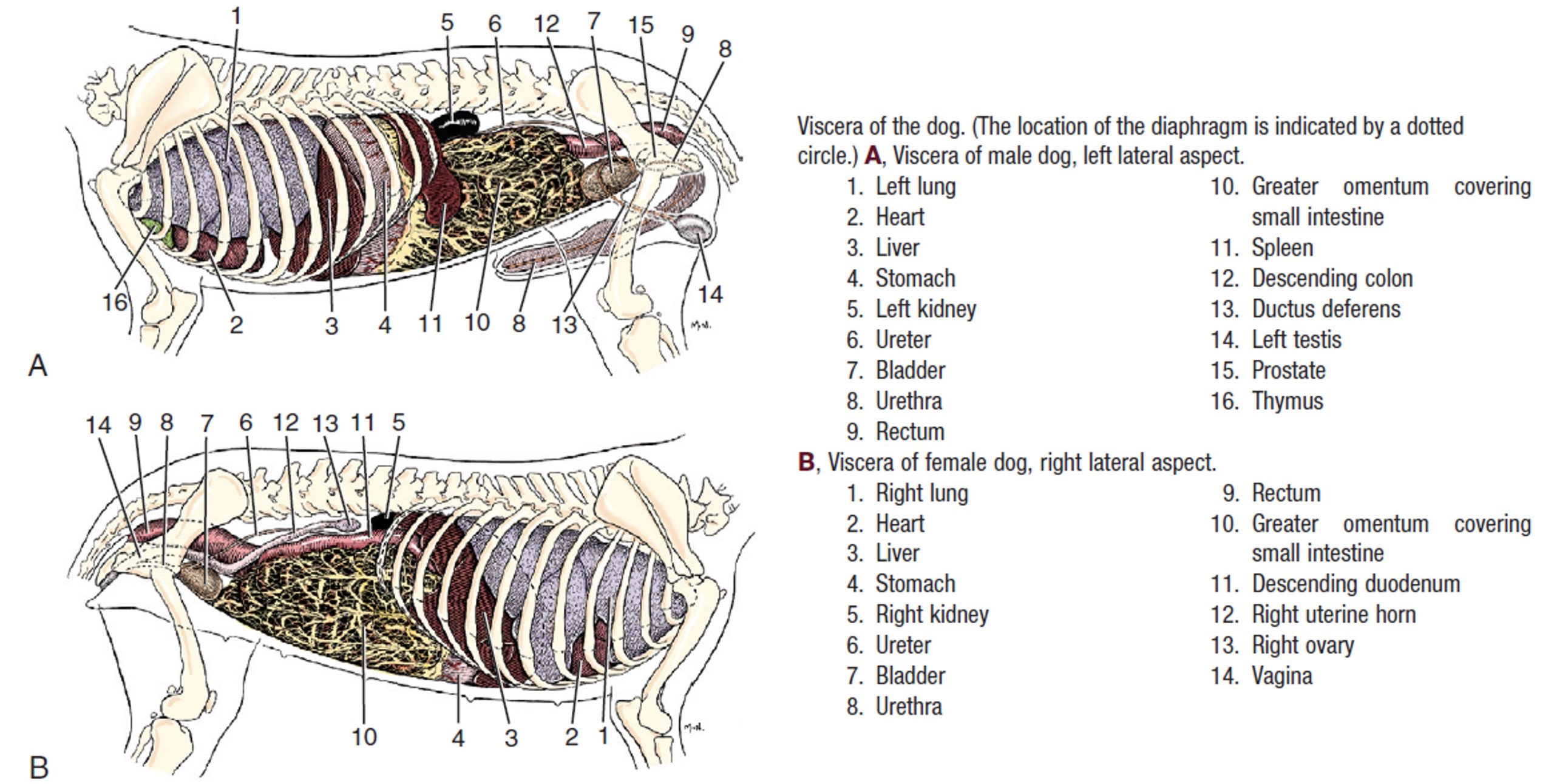
- Viscera of the dog. 1
-
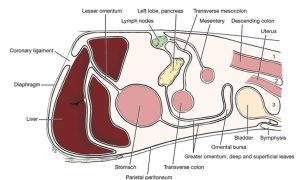
- Diagram of peritoneal reflections, sagittal section. 1
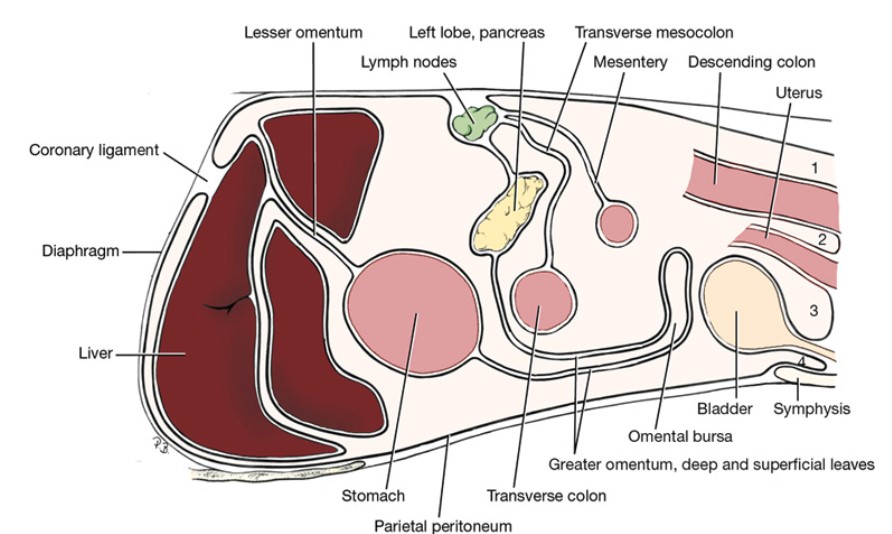
Observe: Follow the greater omentum from its ventral attachment on the greater curvature of the stomach to its dorsal attachment to the dorsal body wall. Reflect the greater omentum away from the underlying viscera and, using your fingers on opposite sides, separate its superficial and deep leaves to expose its cavity, the omental bursa.
The omental bursa, the space between the superficial and deep leaves of the greater omentum, opens to the main peritoneal cavity via the epiploic foramen. This opening lies dorsally to the right of the median plane at the level of the cranial duodenal flexure, caudomedial to the caudate lobe of the liver. It is bounded dorsally by the caudal vena cava, ventrally by the hepatic portal vein, caudally by the hepatic artery in the mesoduodenum, and cranially by the liver.
The epiploic foramen is best observed later in the dissection and will be discussed again when other structures in this region are observed.
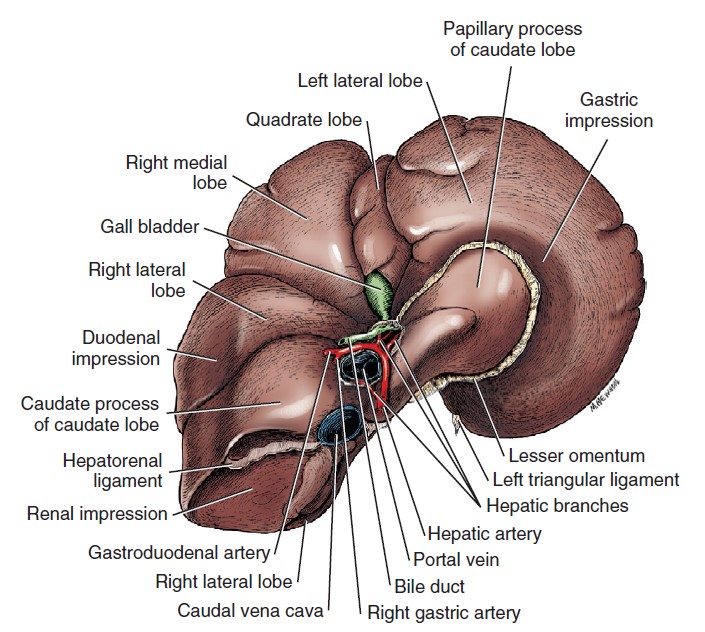
The lesser omentum, a part of the ventral mesogastrium, loosely spans the distance from the lesser curvature of the stomach (the smaller, more cranial curve of the stomach) to the porta of the liver. Between the liver and the cardia of the stomach, it attaches for a short distance to the diaphragm. The papillary process of the liver is loosely enveloped by the lesser omentum. On the right the free edge of the lesser omentum is the hepatoduodenal ligament, which attaches the liver to the duodenum. The hepatoduodenal ligament contains the hepatic portal vein, the hepatic artery, and the bile duct.
-
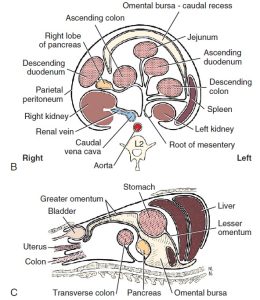
- B. Transverse section through the root of the mesentery. C, Sagittal section. 1
-
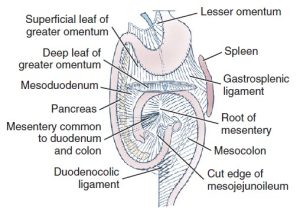
- Plan of visceral and connecting peritoneum, ventral aspect. The greater omentum is transected caudal to the stomach. Arrow in omental bursa. 1
-
- Lesser omentum
-

- Position of the epiploic foramen in the dog. 7
Observe: If possible at this time, observe the lesser omentum attached to the lesser curvature of the stomach running cranially over a small part of the liver called the papillary process of the liver. If it is not visible yet, it can be noted later, during the liver dissection and/or when tracing the vasculature which supplies the liver.
The Spleen
The spleen lies in the superficial leaf of the greater omentum to the left of the median plane along the greater curvature of the stomach. Its position, shape, and degree of distention are variable. Its lateral surface lies against the parietal peritoneum of the left lateral abdominal wall and the liver. Its caudal part may reach to a transverse plane through the mid-lumbar region. Its cranial limit is usually marked by a plane passing between the twelfth and thirteenth thoracic vertebrae. It may reach the floor of the abdomen. The part of the greater omentum that attaches the spleen to the stomach is the gastrosplenic ligament. If your specimen was anesthetized with a barbiturate, the spleen may be abnormally enlarged.
-
- Abdominal viscera of the dog, ventral aspect. 1
Observe: Observe the spleen in your cadaver.
The Diaphragm
The diaphragm, the muscular partition between the thoracic and the abdominal cavities, is a muscle of inspiration. It has an extensive muscular periphery and a small, V-shaped tendinous center. The muscular part of the diaphragm is divided into three parts according to its attachments: lumbar, costal, and sternal. The lumbar part forms the left and right crura that attach to the bodies of the third and fourth lumbar vertebrae by large tendons. The right crus is larger than the left. The costal part of the diaphragm arises from the medial surfaces of the eighth to thirteenth ribs. It interdigitates with the transversus abdominis muscle. The sternal part is narrow and arises from the dorsal surface of the sternum cranial to the xiphoid cartilage. The cupula is the most cranial extent of the dome-shaped diaphragm that bulges into the thorax. The extensions of the V-shaped tendinous center run dorsally between the lumbar and costal parts of each side.
The aortic hiatus is a dorsal passageway between the crura for the aorta, the azygos vein, and the thoracic duct. The more centrally located esophageal hiatus is in the muscular part of the right crus and transmits the esophagus, vagal nerve trunks, and esophageal vessels. The caval foramen is located at the junction of the tendinous and muscular parts of the right side of the diaphragm. The caudal vena cava passes through the caval foramen.
-
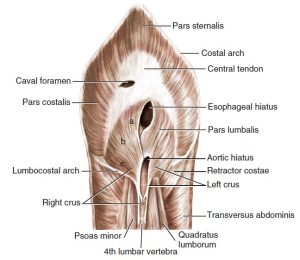
- Abdominal surface of the diaphragm. 1
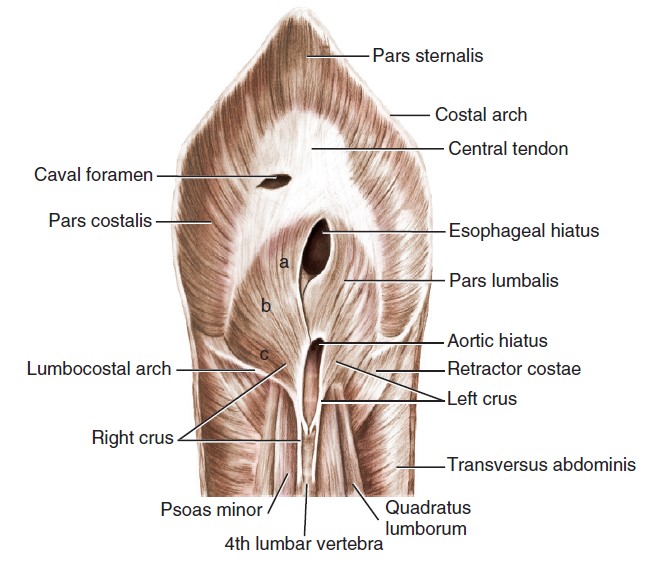
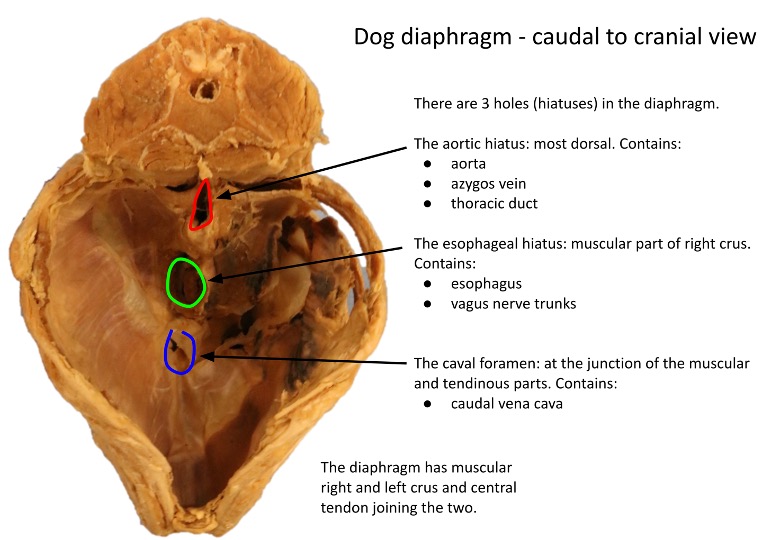
Observe: On the left side of the cadaver, incise the muscular periphery of the diaphragm approximately a half-inch from its costal attachments. Observe esophageal and aortic hiatuses. The caval foramen need not be directly observed in the cadaver.
The Liver and Gallbladder
Observe: Observe the liver, its parts and biliary structures as described below, both in situ and ex situ (unless otherwise stated).
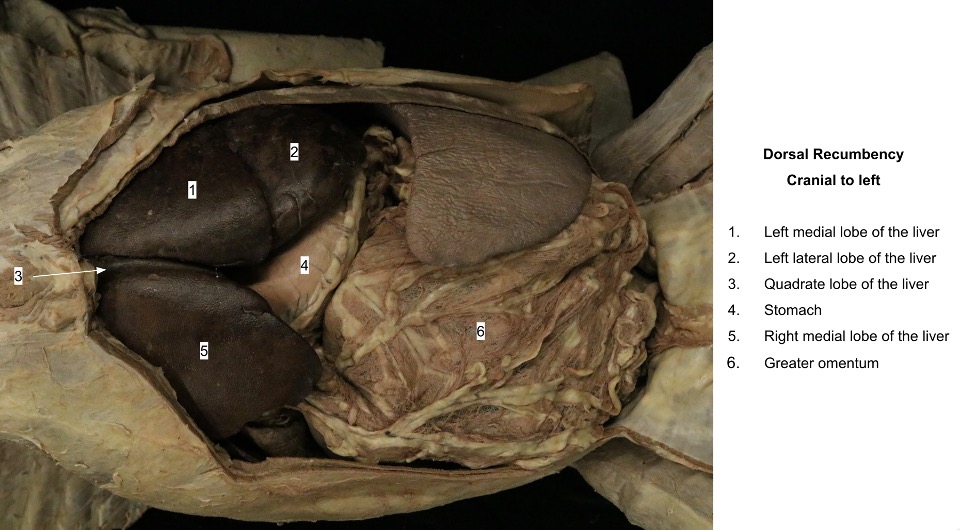
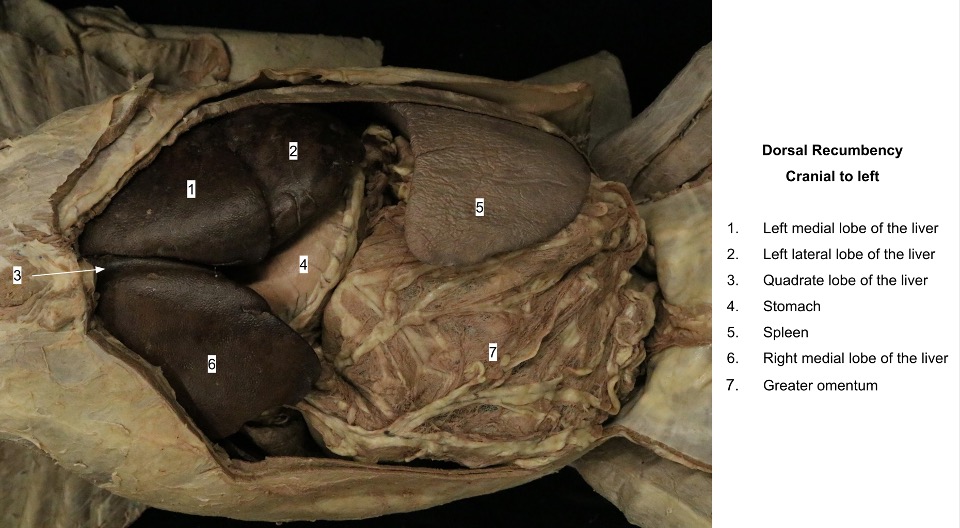
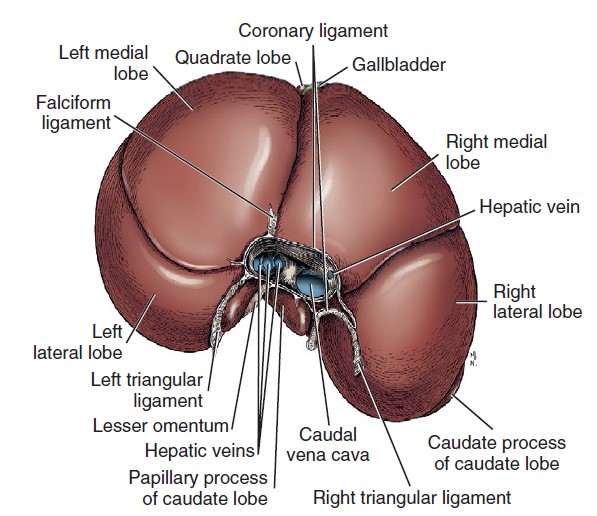
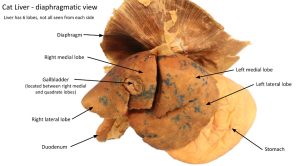
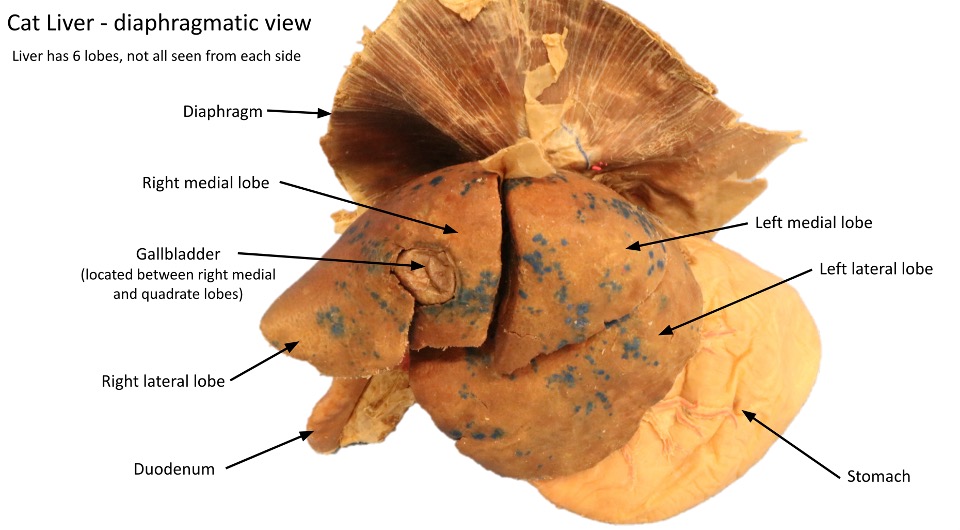
The liver has 4 major lobes, right, left, quadrate and caudate, with some of these lobes subdivided. The liver’s parietal (i.e., cranial) surface conforms to the abdominal surface of the diaphragm. The visceral surface of the liver is related on the left to the stomach and sometimes to the spleen; on the right to the pancreas, right kidney, and duodenum; and ventrally to the greater omentum and through this to the small intestine. Its most caudal part (the renal impression of the caudate process of the caudate lobe of the liver, see below) covers the cranial extremity of the right kidney, and reaches a transverse plane through the thirteenth thoracic vertebra. The liver rarely projects caudal to the costal arch. It undergoes slight longitudinal movement with each respiration. The liver has peritoneal attachments, some already reviewed.
Ventrally, right and left parts of the coronary ligament converge to form the falciform ligament (previously discussed) which continues to the umbilicus, attached to the ventral body wall. In adult dogs the falciform ligament is filled with fat, and it persists only from the diaphragm to the umbilicus. The round ligament of the liver (previously discussed) lies in the free edge of the falciform ligament.
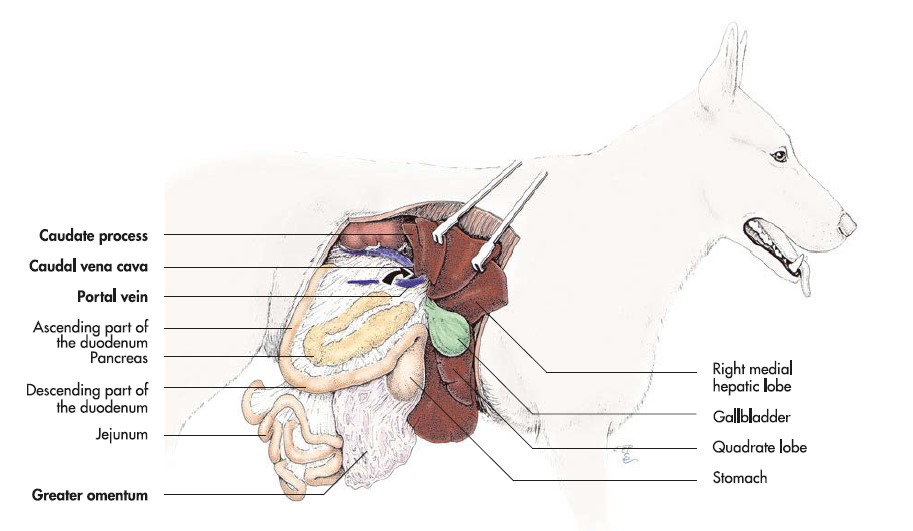
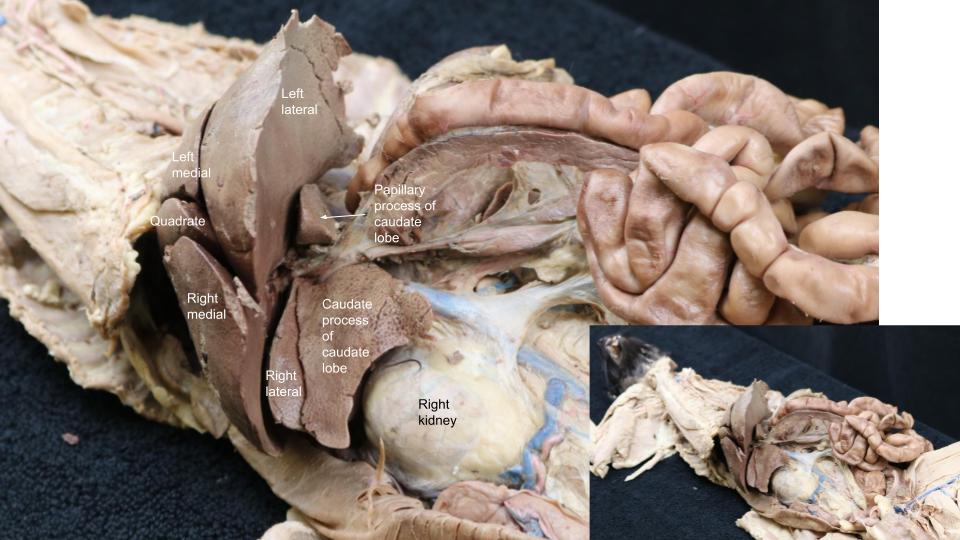
The right and left lobes of the liver are each subdivided into medial and lateral parts. The right medial lobe contains a fossa for the gallbladder. The right lateral lobe, which is smaller, is located next to the caudate lobe, which embraces the cranial end of the right kidney via its caudate process. The quadrate lobe is narrow and is located between the right and left medial lobes. It forms the left boundary of the fossa of the gallbladder. The left medial lobe is separated by a fissure from the right medial and quadrate lobes. The umbilical vein enters the liver through this fissure. The left lateral lobe is separated by a fissure from the left medial lobe. The free margin of the left lateral lobe is frequently notched. The visceral surface of the left lateral lobe is concave where it contacts the stomach.
The caudate lobe is indistinctly separated from the central mass of the liver, which is cranial to it. It lies transversely, but it is mainly to the right of and dorsal to the main bulk of the organ. It is constricted in its middle where the portal vein enters the liver ventral to it and the caudal vena cava crosses dorsal to it. Its extremities are in the form of two processes. The caudate process caps the cranial end of the right kidney and thus contains the deep renal impression. The papillary process can be seen through the lesser omentum if the liver is tipped forward. It lies in the lesser curvature of the stomach.
-
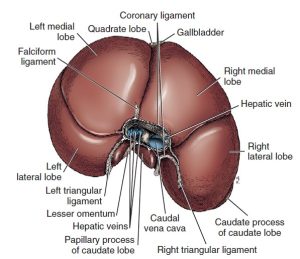
- Liver of the dog, diaphragmatic aspect. 1
-
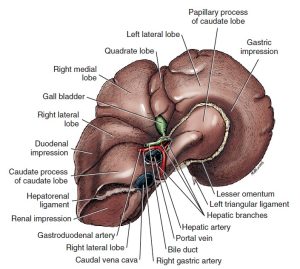
- Liver of the dog, visceral aspect. 1
-
- Bile, hepatic, and pancreatic ducts. 1
-
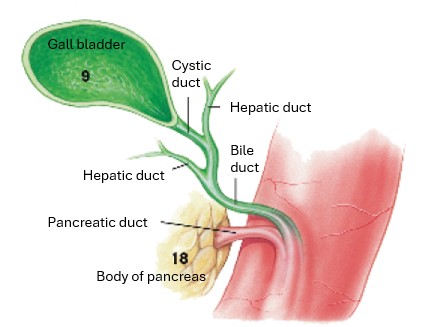
- Gallbladder and bile duct of the cat, dorsal view. 4
-
- Cat liver
-
- Cat liver
Observe: Using the liver in your cadaver and the wet specimens made available to you in the lab, identify the different lobes of the liver.
Also recall that the epiploic foramen is the only natural opening into the omental bursa, which is the space located between the superficial and deep leaves of the greater omentum. It is caudomedial to the caudate lobe of the liver and is bounded dorsally by the caudal vena cava, ventrally by the (non-latexed) hepatic portal vein, caudally by the hepatic artery in the mesoduodenum, and cranially by the liver.
Observe: To observe the epiploic foramen, find the caudate process of the caudate lobe with its renal impression. Place a finger directly ventral to the caudate process of the caudate lobe and rest it on the structures directly ventral to it, listed above. Your finger should be pointing into or near the epiploic foramen.
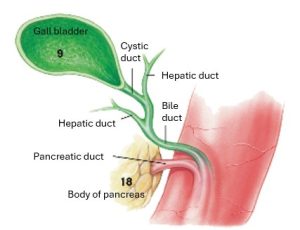
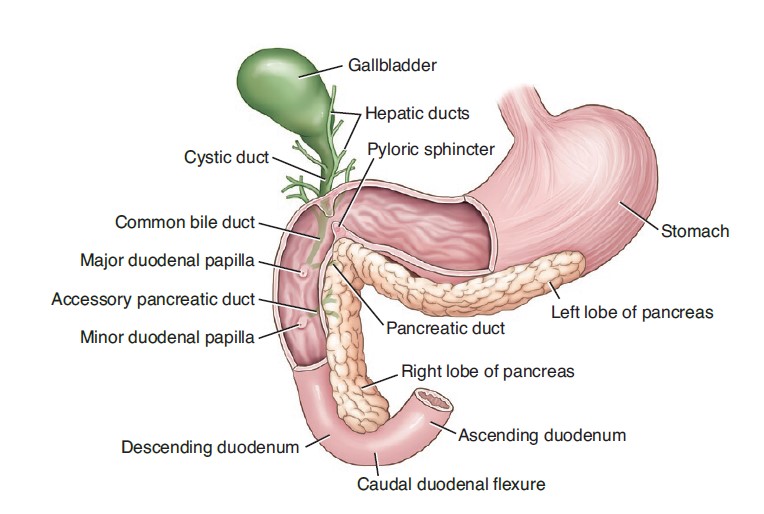
The gallbladder is located in a fossa between the quadrate and right medial lobes of the liver. A full gallbladder extends through the liver and contacts the diaphragm (which is often stained green in preserved specimens). The neck of the gallbladder is continued as the cystic duct.
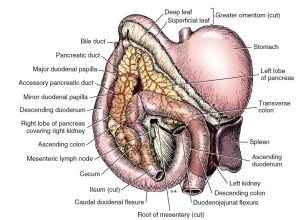
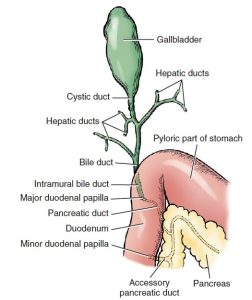
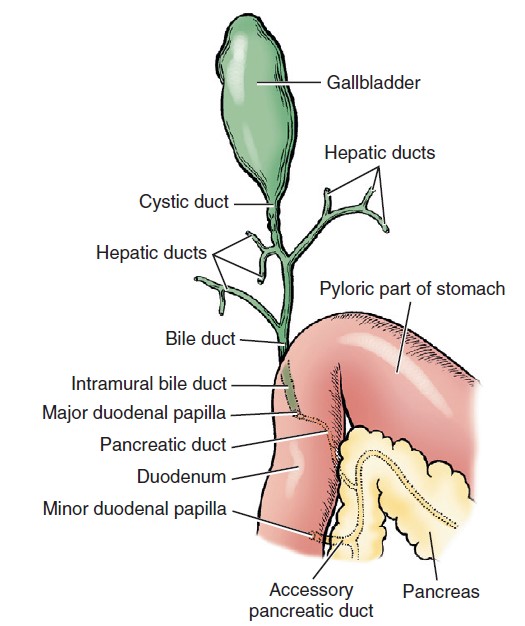
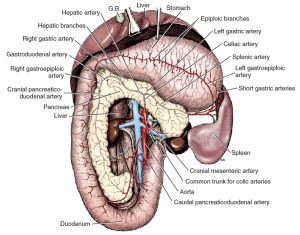
The main duct formed by the union of the hepatic ducts and the cystic duct from the gallbladder is the bile duct. It courses through the wall of the descending duodenum and terminates on the major duodenal papilla alongside the pancreatic duct. There are no valves in the biliary ducts, and bile may flow in either direction.
Observe: Observe the gallbladder and cystic duct on wet liver specimens.
The Stomach
Observe: Observe the structures of the stomach described below in your cadaver, as well as on prosected cadavers and wet specimens and plastinated models.
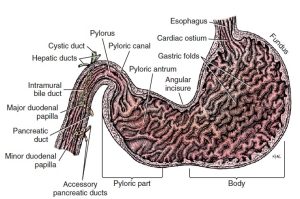
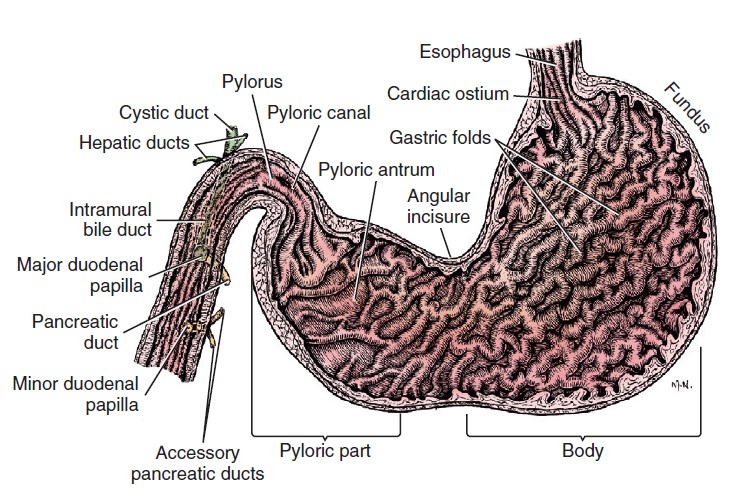
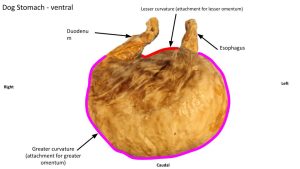
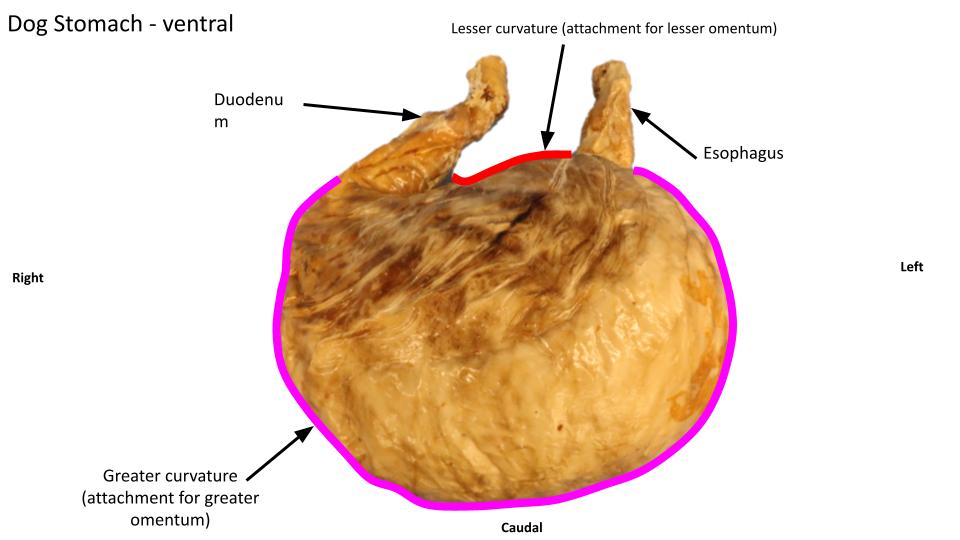
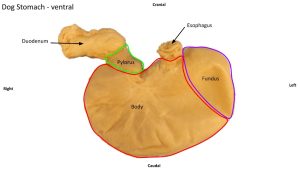
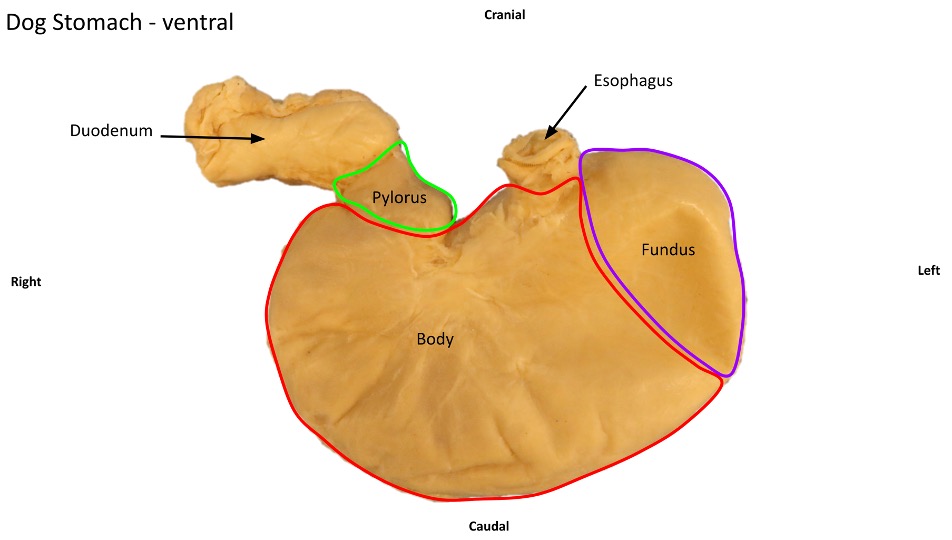
The stomach is divided into parts that blend imperceptibly with one another. The cardiac part is the smallest part of the stomach and is situated nearest the esophagus. The fundus is dome-shaped and lies to the left of and dorsal to the cardia (i.e., where the esophagus enters the stomach). The body of the stomach is the large middle portion. It extends from the fundus on the left to the pyloric part on the right. The body joins the pyloric part at the angular incisure, which is the relatively sharp bend on the lesser curvature. The pyloric part is the distal third of the stomach as measured along the lesser curvature. The initial thin-walled portion is the pyloric antrum, which narrows to a pyloric canal before joining the duodenum at the pyloric sphincter ( i.e. the pylorus.)
The stomach is bent so that its greater curvature faces mainly to the left, caudally and ventrally. This curvature lies above and to the left of the mass of the small intestine. The lesser curvature faces mainly to the right, and craniodorsally, and is strongly curved around the papillary process of the liver; the left lobe of the pancreas and transverse colon are dorsocaudal to it. The parietal surface of the stomach faces cranioventrally toward the liver, and its visceral surface faces caudodorsally toward the intestinal mass. Its position changes depending on its fullness. The empty stomach is completely hidden from palpation and observation by the liver and diaphragm cranioventrally and the intestinal mass caudally. It lies to the left of the median plane. The empty stomach is cranial to the costal arch and sharply curved, so that it is more V-shaped than C-shaped. The full stomach lies in contact with the ventral abdominal wall and protrudes beyond the costal arches. It displaces the intestinal mass.
-
- Longitudinal section of stomach and proximal portion of duodenum. 1
-
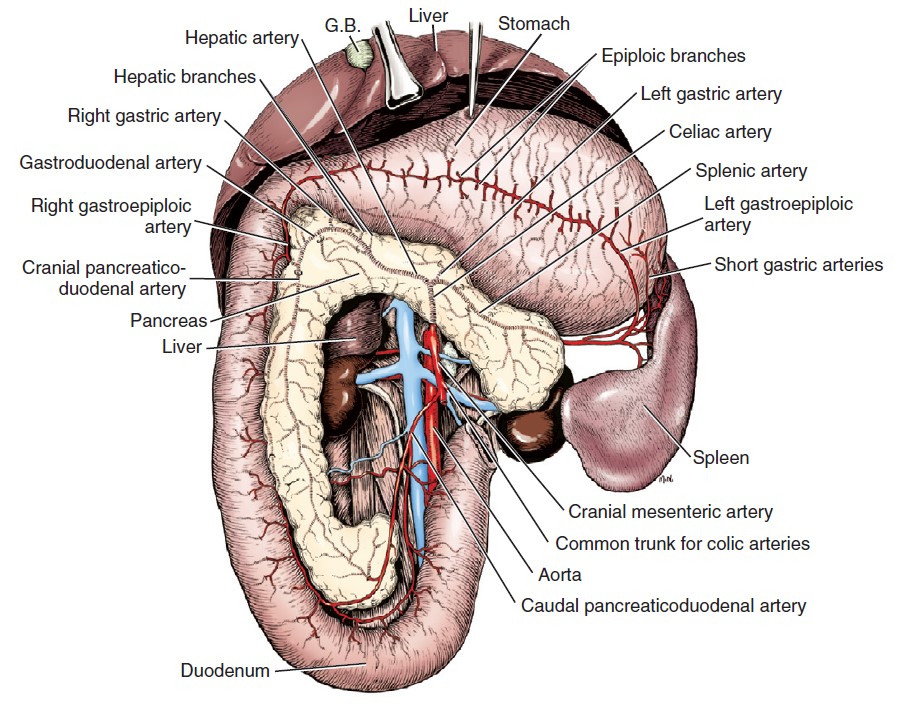
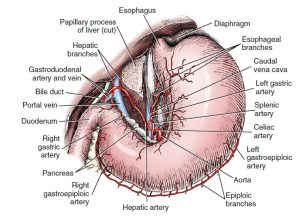
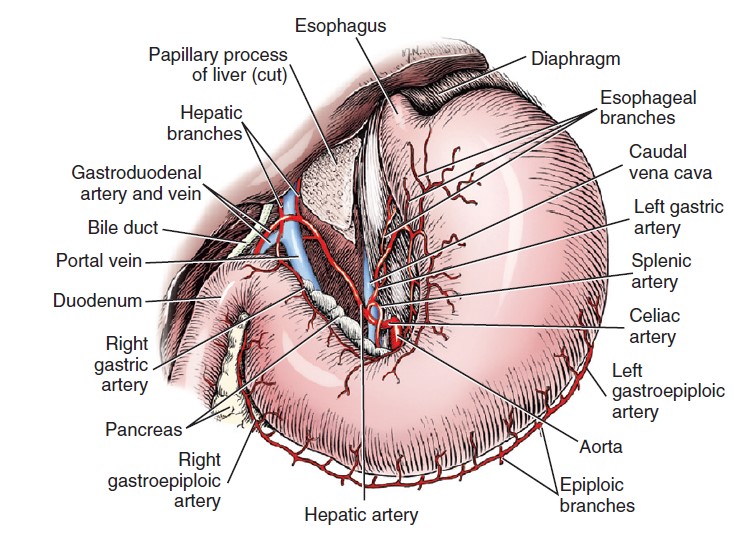
- Celiac and cranial mesenteric arteries, ventral aspect. (Stomach reflected cranially.) 1
-
- Celiac artery, ventral aspect. (Stomach displaced to left.) 1
-
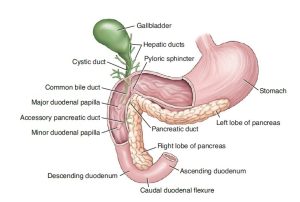
- Normal canine anatomy of the extrahepatic biliary system and pancreas. 9
-
- Dog stomach
-
- Dog stomach
Dissect: Incise the stomach on its ventral surface, in between the greater and lesser curvatures of the stomach (i.e. the part lacking substantial vasculature. This is where gastrostomies are typically performed so as to avoid major vessels.). Empty the stomach contents into the table buckets to observe the longitudinal folds of mucous membrane (the rugae) lining the stomach. Observe the longitudinal folds of mucous membrane (the rugae), on prosected cadavers, and/or on wet specimens and plastinated models.
Clinical application: GASTRIC DILATATION AND VOLVULUS (GDV)
Gastric dilatation and volvulus is an acute, life-threatening condition. It most commonly occurs in large, deep chested dogs including the German Shepherd, Standard Poodle, Great Dane, Boxer, Doberman Pinscher, Saint Bernard, and Irish Setter. It is most common in middle-age to older dogs. Etiologic factors associated with GDV include anatomic predisposition, hereditary factors, food-filled
stomach with postprandial exercise, large amounts of water consumption, and weakened gastric supportive ligaments. Risk factors associated with gastric dilatation are general anesthesia, aerophagia, high anxiety level, overeating, and gastric and duodenal obstruction. With GDV, the stomach moves in a clockwise direction as viewed ventrodorsally and caudally. The degree of rotation usually ranges from 90 to 360 degrees, and occasionally rotates up to 540 degrees.
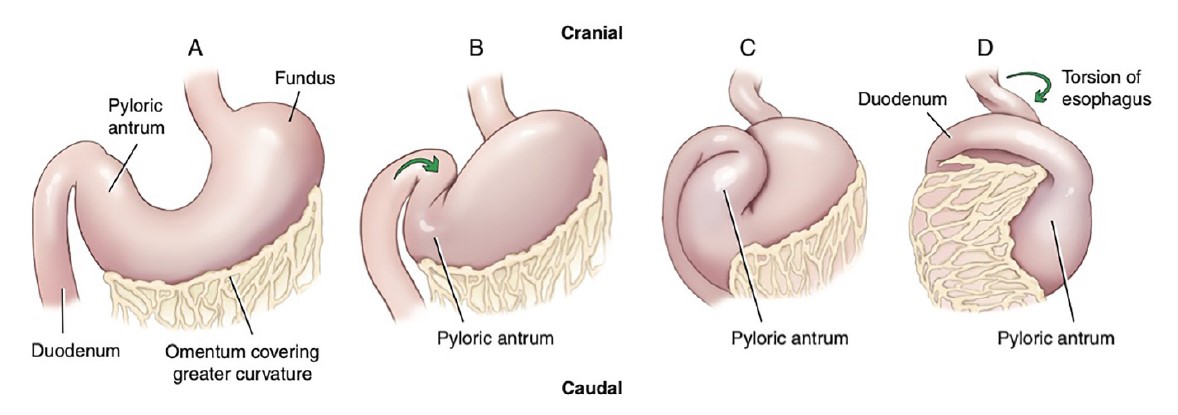
(A) The normal position of the esophagus, stomach, pylorus, and duodenum.
(B) The pylorus rotates ventrally and laterally to the body of the stomach.
(C) The pylorus moves upward, crossing the distended stomach toward the left abdominal wall and stretching the duodenum across the cardia as it crosses the midline.
(D) The fundic part of the stomach moves dorsally, the greater curvature is displaced ventrally, and the ventral leaf of the greater omentum covers the ventral aspect of the stomach.
This results in a clockwise torsion of the esophagus with the duodenum displaced to the left.
Review videos
Peritoneum, omentum and ligaments w/ Dr. Gerard – 21 min
Peritoneum, omentum and stomach w/ Dr. Walker – 7 min, watch until 17 min
Cat stomach – 2 min, watch until 2 min
Carnivore liver and bladder ligaments – 5 min, watch until 29 min
Terms
| Term | Species/Notes |
| Peritoneal cavity | Carnivore |
| Parietal peritoneum | Carnivore |
| Transversalis fascia | Carnivore |
| Connecting peritoneum | Carnivore |
| Mesoduodenum | Carnivore |
| Mesojejunum | Carnivore |
| Mesocolon | Carnivore |
| Greater omentum | Carnivore |
| Superficial leaf | Carnivore |
| Deep leaf | Carnivore |
| Omental bursa | Space between superficial and deep leaves |
| Epiploic foramen | ID; know boundaries |
| Lesser omentum | Carnivore |
| Falciform ligament | Carnivore |
| Round ligament of the liver | Carnivore; free edge of falciform lig. |
| Umbilical vein | Fetal structure which degenerates to round lig. of liver |
| Median ligament of bladder | Carnivore |
| Spleen | Carnivore |
| Diaphragm | Carnivore |
| Left and right crus | Carnivore |
| Esophageal hiatus | Carnivore |
| Aortic hiatus | Carnivore |
| Caval foramen | Carnivore |
| Liver | Carnivore |
| Right medial lobe | Carnivore |
| Right lateral lobe | Carnivore |
| Quadrate lobe | Carnivore |
| Caudate lobe | Carnivore |
| Caudate process | Carnivore |
| Papillary process | Carnivore |
| Renal impression | Carnivore |
| Left medial lobe | Carnivore |
| Left lateral lobe | Carnivore |
| Gallbladder | Carnivore |
| (Common) bile duct | Carnivore |
| Major duodenal papilla | Identify in the duodenum |
| Stomach | Carnivore |
| Greater curvature | Carnivore |
| Lesser curvature | Carnivore |
| Fundus | Carnivore |
| Body | Carnivore |
| Pylorus | Carnivore |
| Pyloric sphincter | Ring of muscle separating stomach from duodenum |